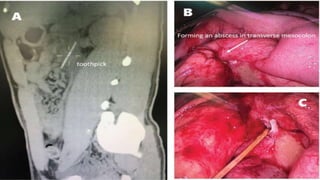
Gastrointestinal perforation can be caused by a variety of illnesses and medical conditions that damage the intestinal wall such as appendicitis, diverticulitis, ulcers, gallstones, inflammatory bowel diseases, abdominal trauma, surgery, and foreign object ingestion. Symptoms include severe abdominal pain, fever, nausea, vomiting, and rectal bleeding. Diagnosis involves x-rays, CT scans, and lab tests. Treatment is usually surgery to repair the perforation and address underlying causes, though sometimes antibiotics alone may be used if the perforation has closed. Complications can include bleeding, infection, abscesses, and permanent colostomies. Prognosis depends on early diagnosis and treatment as well as individual risk factors