
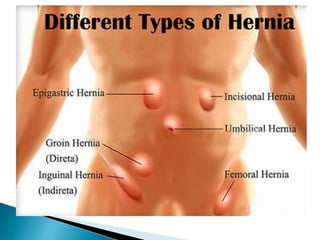

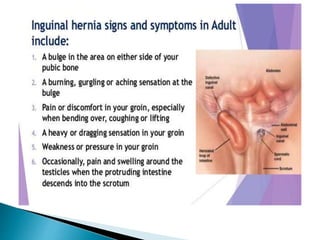
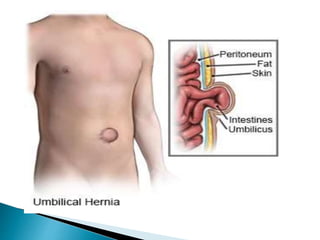
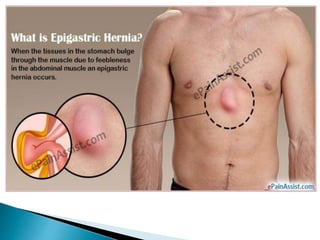
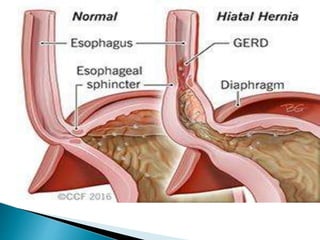
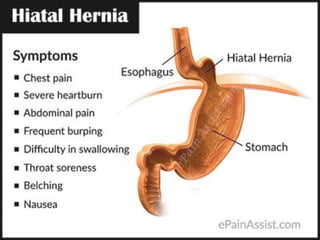
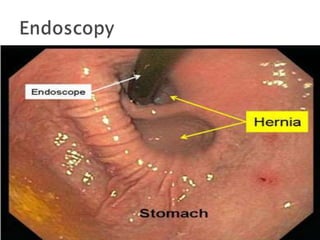
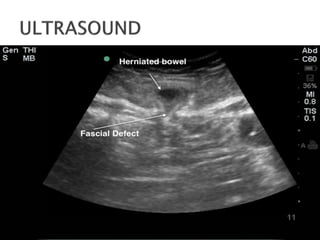
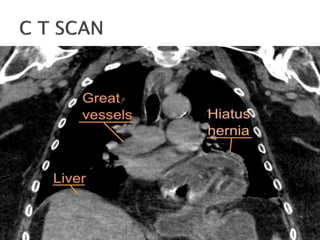
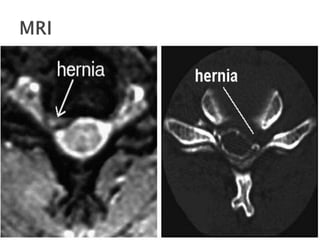

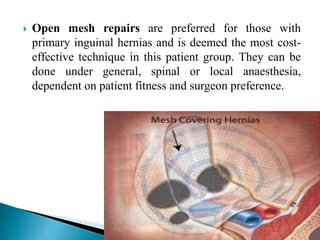
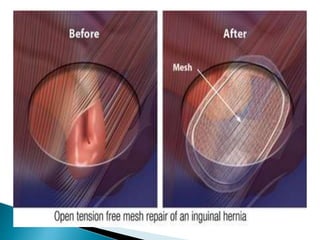





A hernia is an abnormal protrusion that often causes swelling and pain, with abdominal wall hernias affecting 1.7% of all ages and inguinal hernias making up the majority. Risk factors include family history, obesity, and certain physical strains, while types of hernias include femoral, umbilical, and hiatal, each with varying symptoms and treatments. Surgical repair options include open and laparoscopic techniques, with preventive measures focusing on weight management and lifestyle modifications.























































































