Intestinal obstruction is a serious condition that prevents normal movement of digestive products and can affect either the small or large bowel, requiring immediate treatment and possibly surgery. It can be classified into mechanical, non-mechanical, and pseudo-obstruction types, with various causes including adhesions and tumors. Symptoms may include abdominal pain, distention, and constipation, with diagnostic measures including imaging and physical examination to guide management, which may involve decompression and surgical intervention.

![CLASSIFICATION
Dynamic/ Adynamic
Small bowel obstruction [ high or low ]
Large bowel obstruction
Acute
Chronic
Acute on chronic
Subacute
Simple - (no vascular impairment)
Strangulated
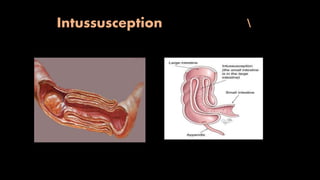
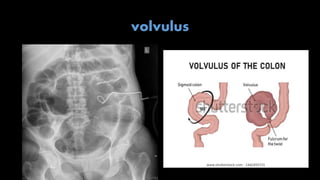
Closed loop obstruction- ( both ends are obstructed e.g volvulus)](https://image.slidesharecdn.com/intestinalobstruction-200429162311/85/Intestinal-obstruction-8-320.jpg)