Downloaded 1,574 times




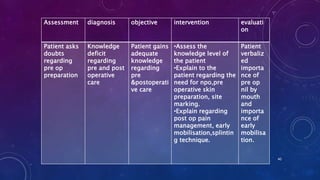
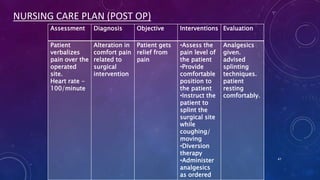
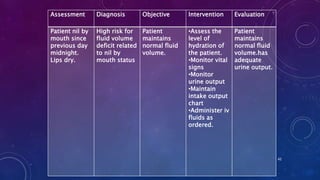
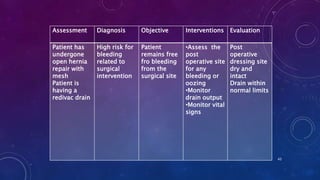
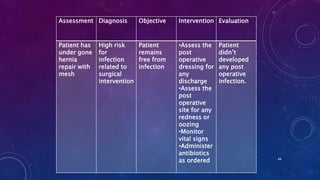
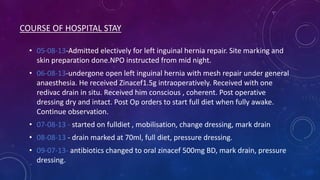
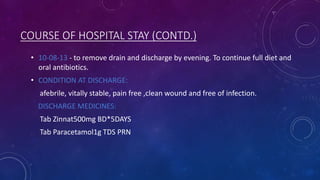
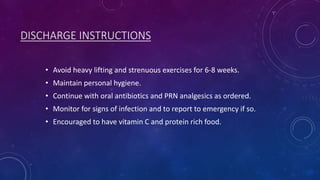


This case study discusses inguinal hernias, detailing their definition, incidence, types (direct and indirect), etiology, signs, symptoms, and management options, including conservative and surgical interventions. It also highlights patient demographics, surgical history, nursing management, and postoperative care for a male patient undergoing open inguinal hernia repair. The conclusion emphasizes the prevalence and surgical treatment of inguinal hernias, which can affect individuals of any age, particularly males.



































































