Downloaded 443 times








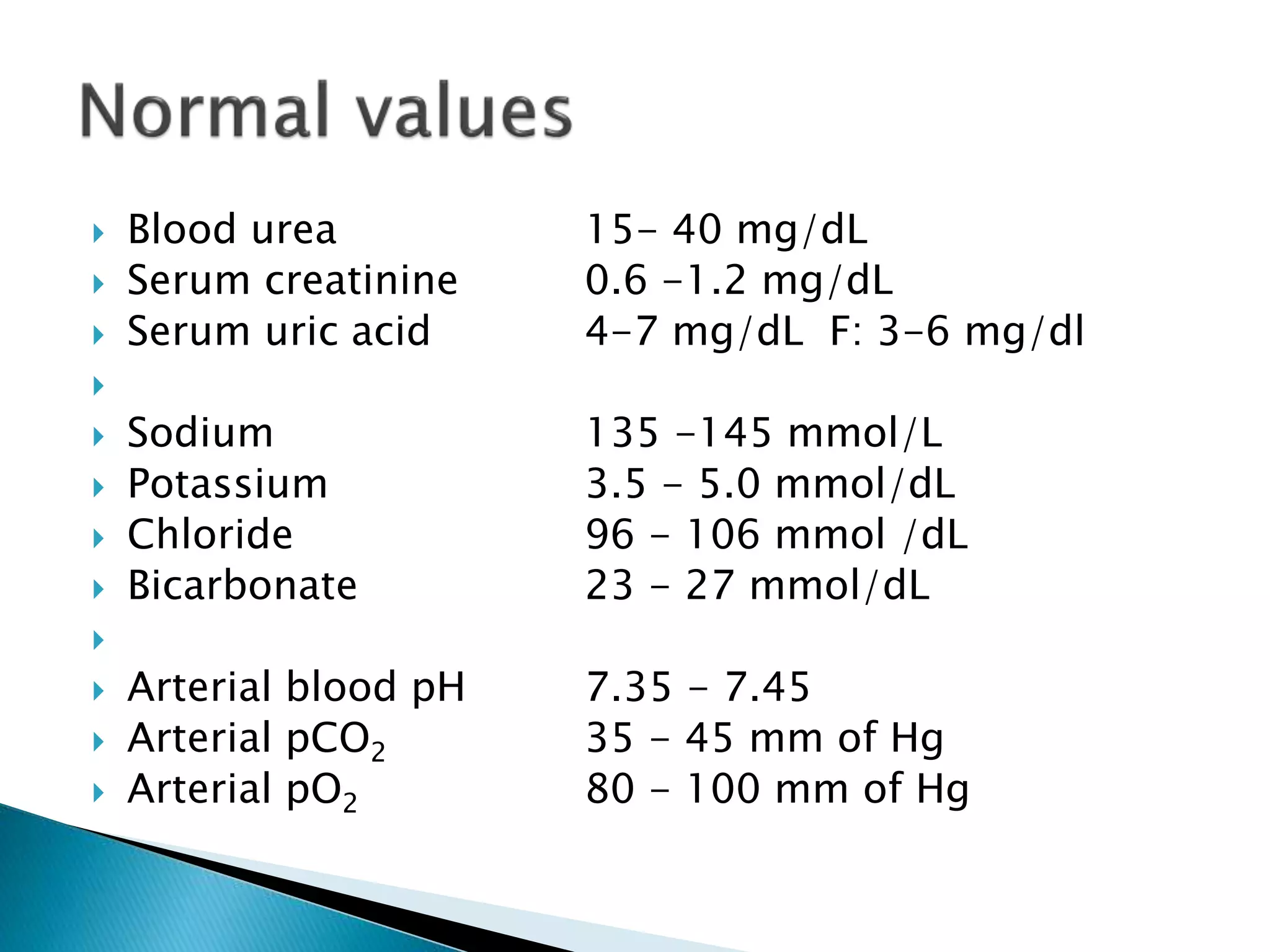

The document discusses the functions and tests of the kidney. It notes that the kidney excretes waste, maintains water and electrolyte balance, and produces hormones. It describes renal clearance tests to assess glomerular and tubular function, including creatinine clearance and urine concentration tests. Normal ranges are provided for various blood and urine parameters. Renal function tests evaluate glomerular filtration rate and tubular function.









































































































