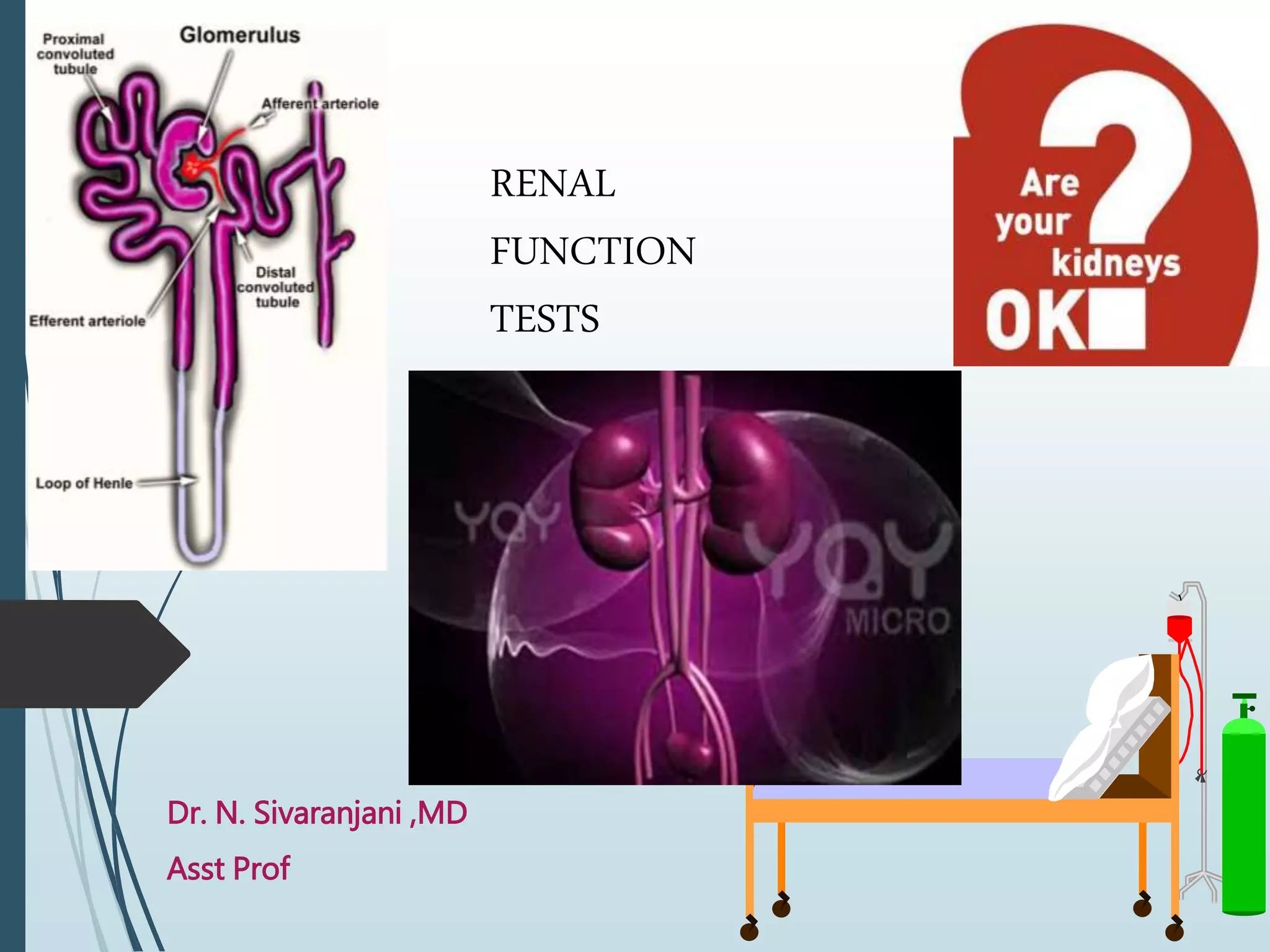
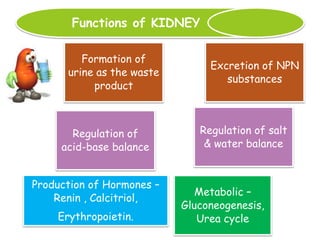
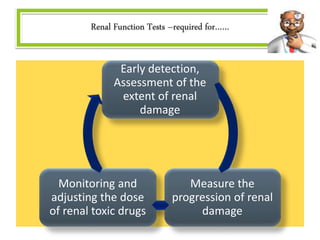
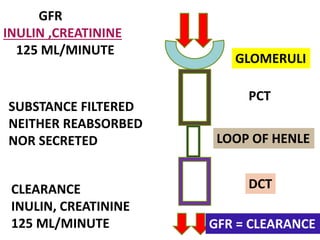
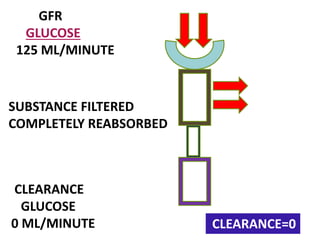
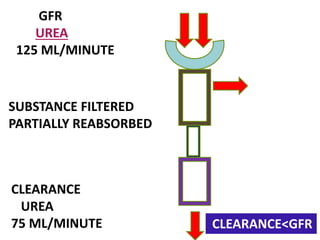
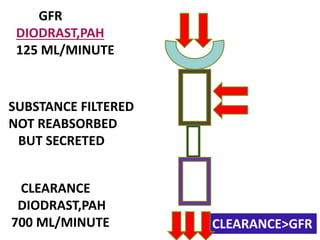
The document provides a comprehensive overview of renal function tests (RFTs) and the kidney's roles, including waste excretion, regulation of bodily fluids, and hormone production. It covers the assessment of glomerular and tubular functions, classification of renal diseases, and the significance of various biochemical markers like serum creatinine and urea for evaluating kidney function. Additionally, it highlights the importance of early detection and monitoring of renal damage, along with practical testing methodologies for assessing renal health.