Downloaded 7,280 times

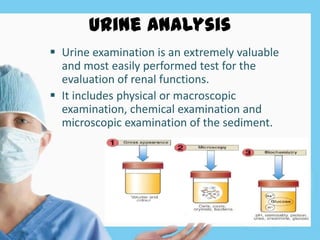










This document discusses renal function tests and their importance in assessing kidney function. It covers urine analysis including physical, chemical and microscopic examination. It also discusses various blood tests like serum creatinine, blood urea, uric acid and electrolytes to evaluate glomerular function. Tests of tubular function examined include urine concentration, vasopressin and water load tests. The significance of renal function tests in acute kidney injury is also highlighted. An addendum discusses cystatin C as a novel marker for non-invasive estimation of glomerular filtration rate and early renal impairment.