Downloaded 251 times

































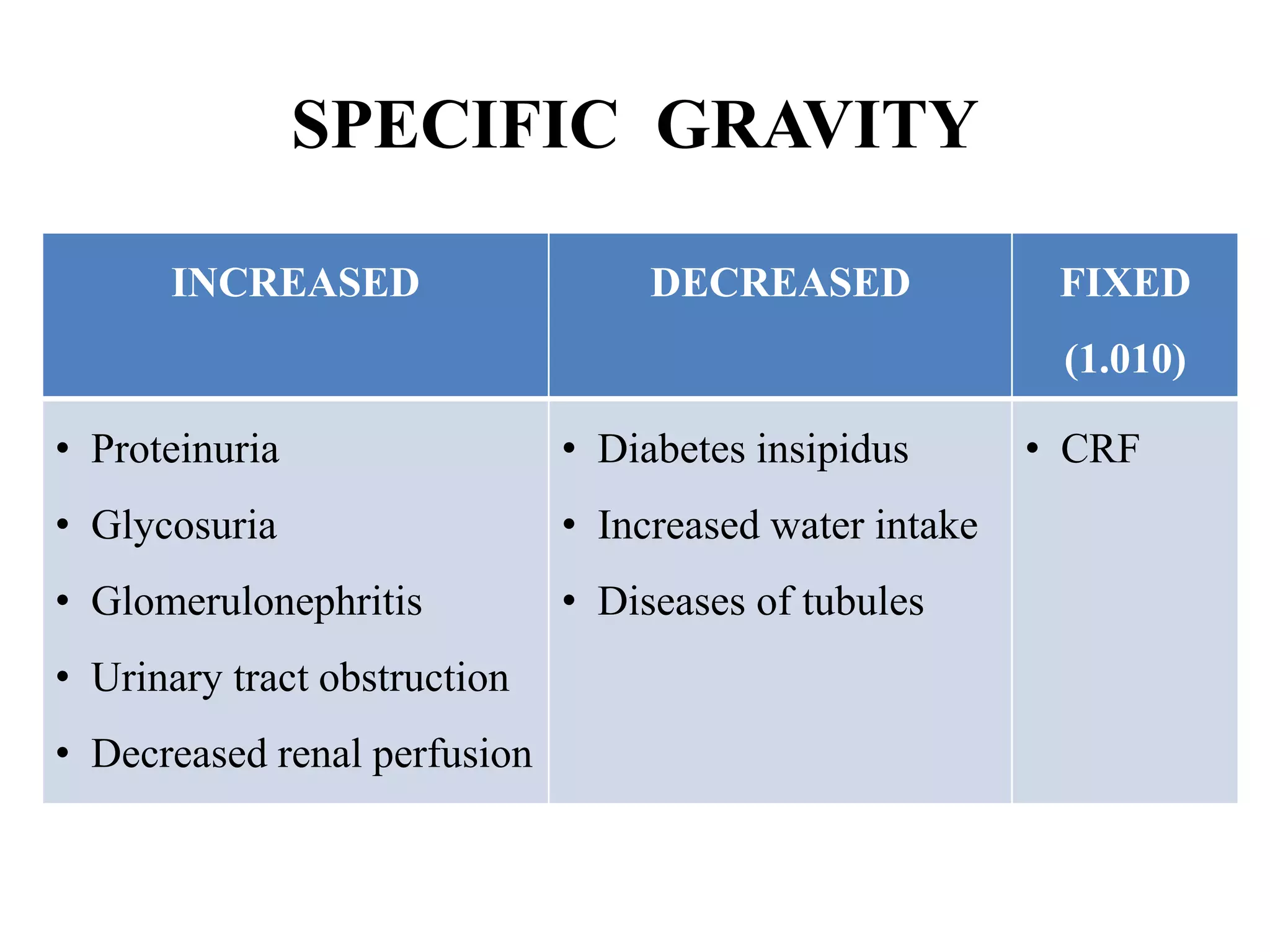









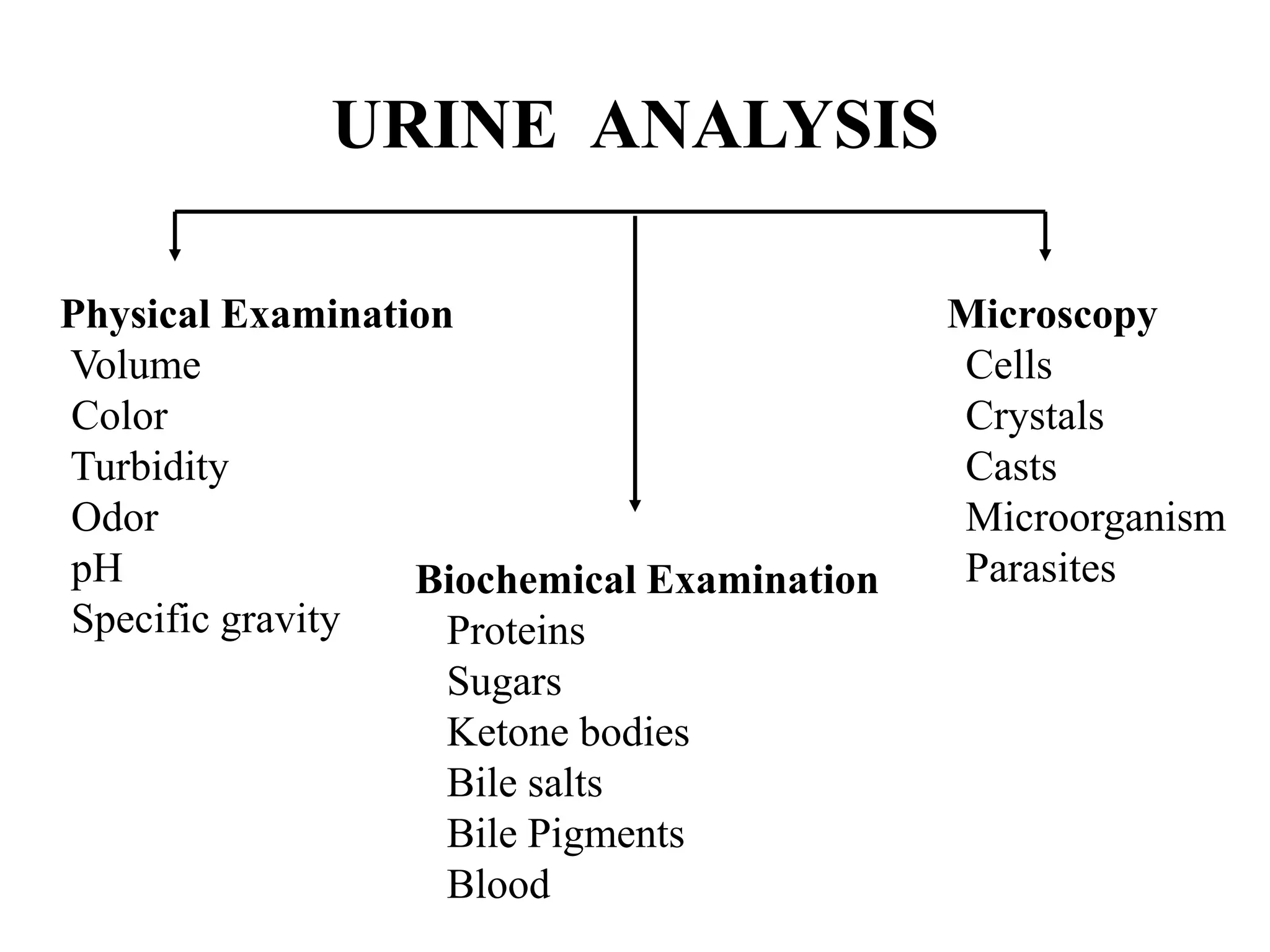





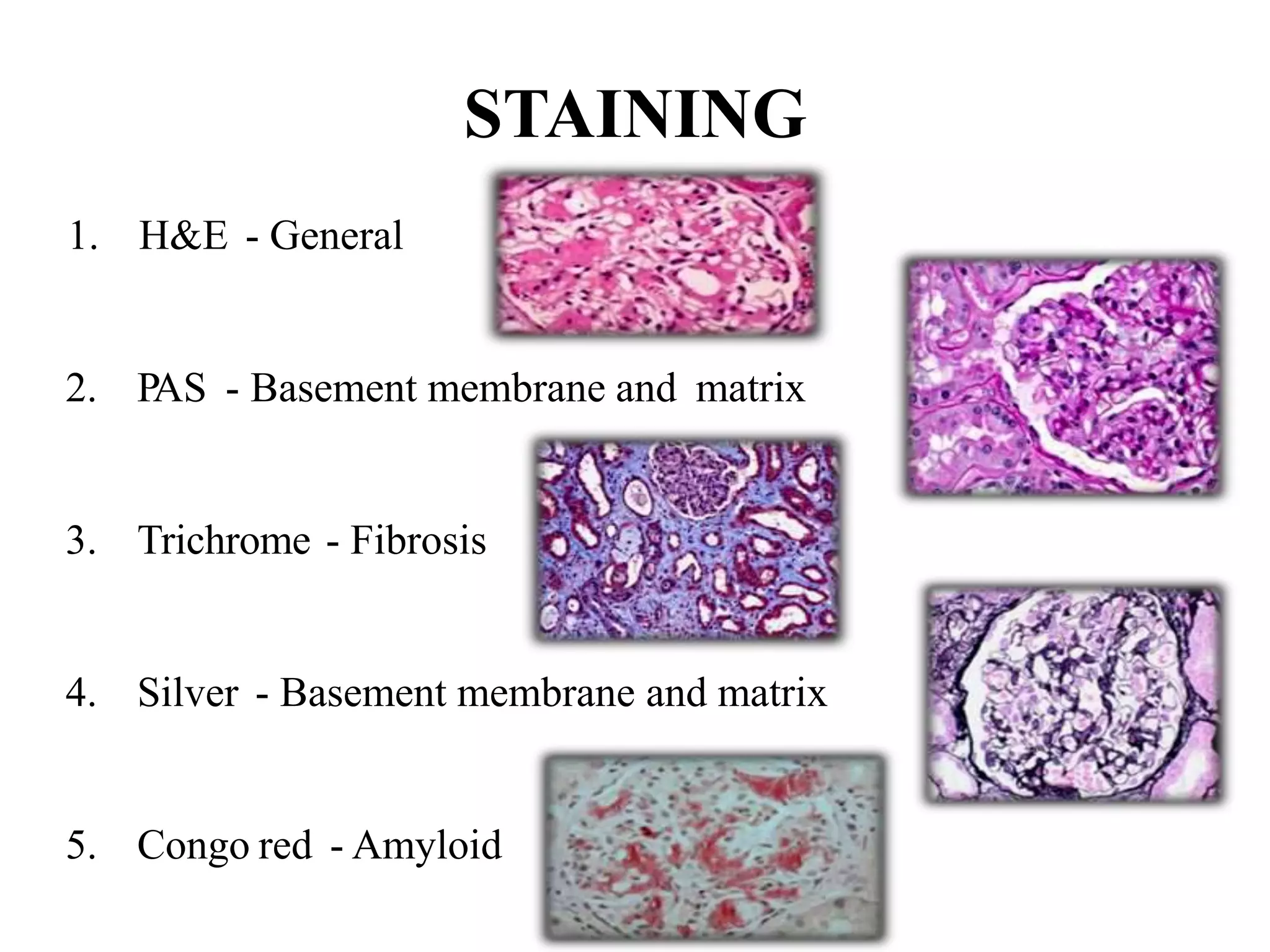


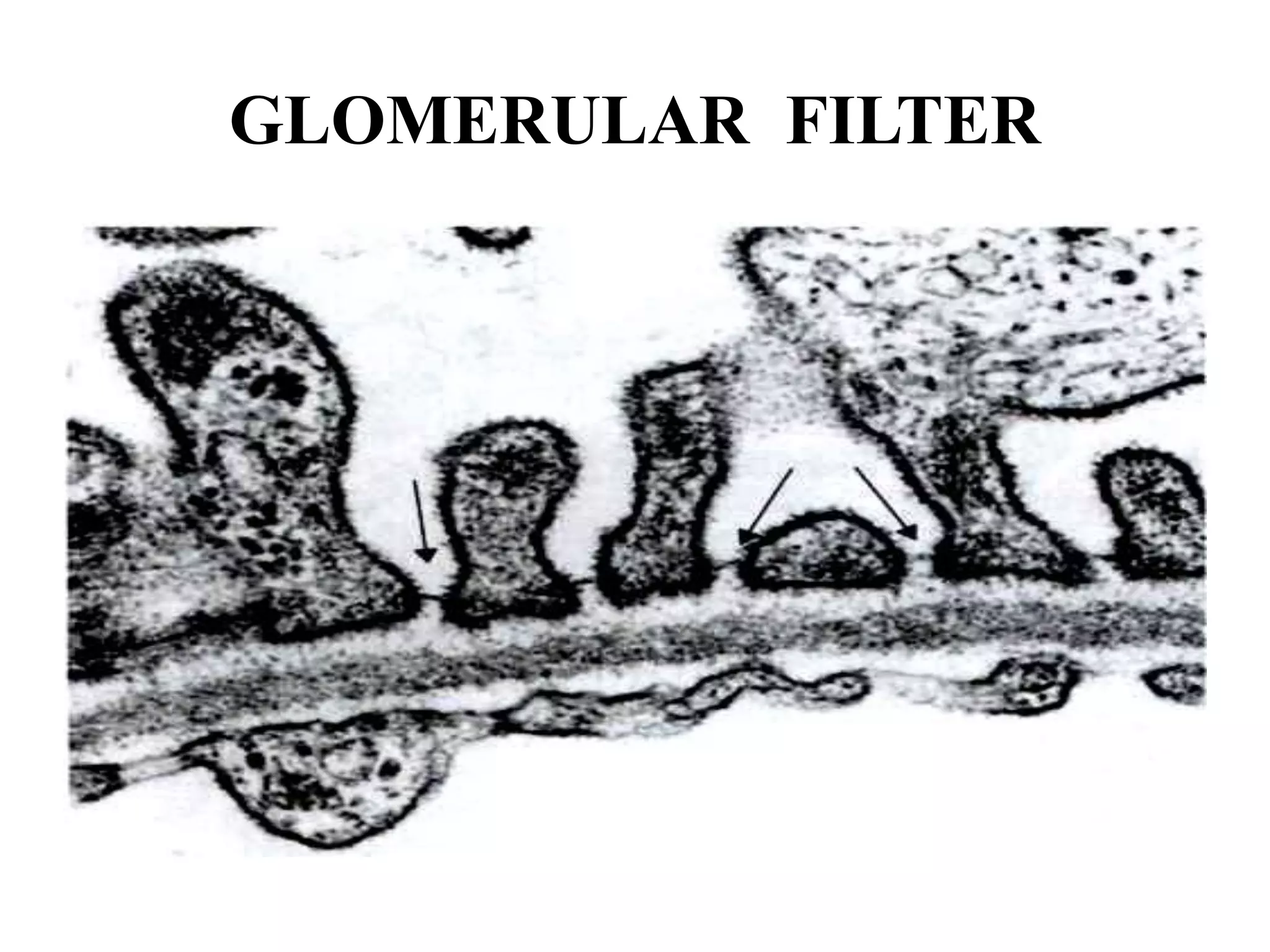



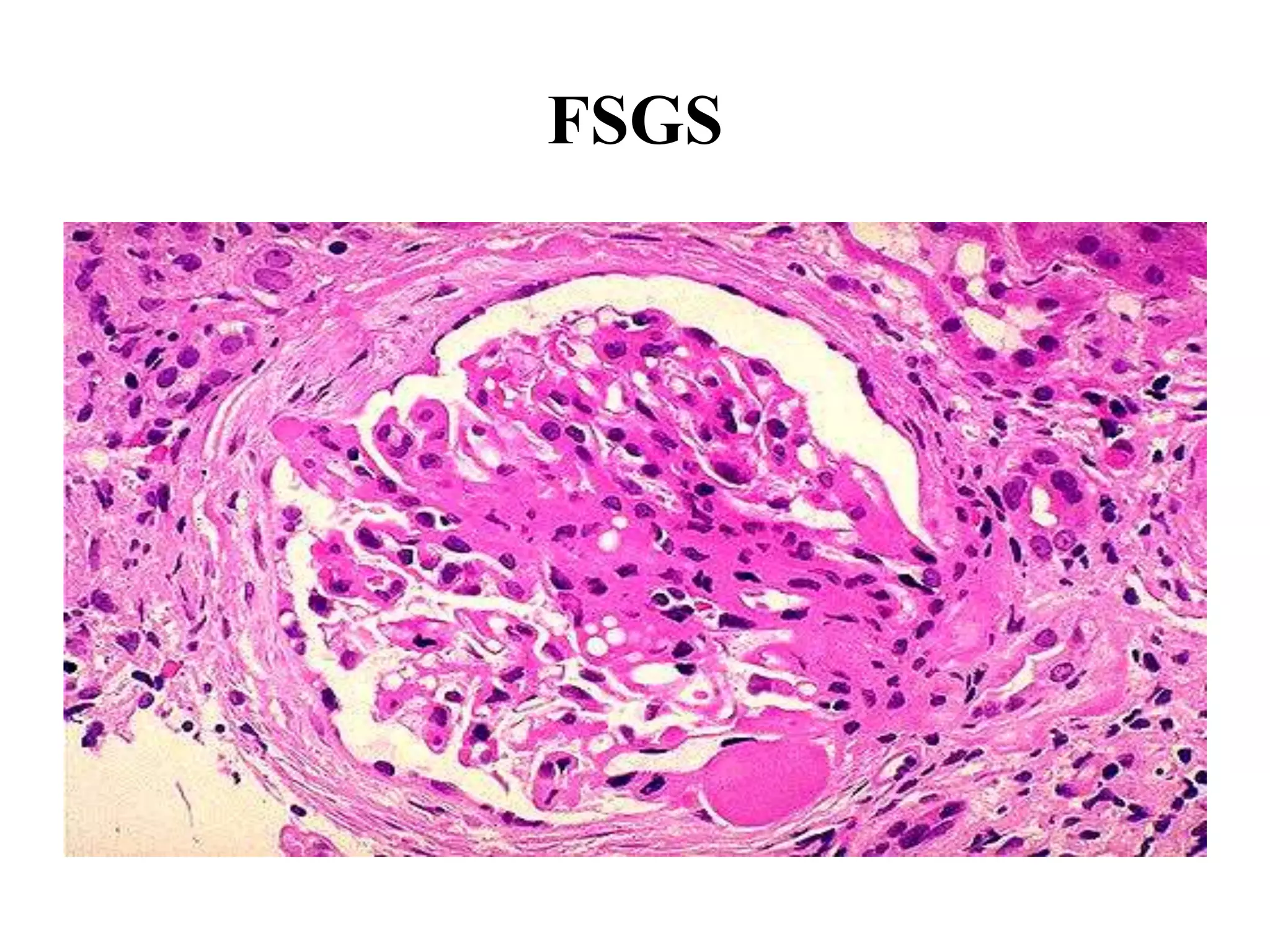

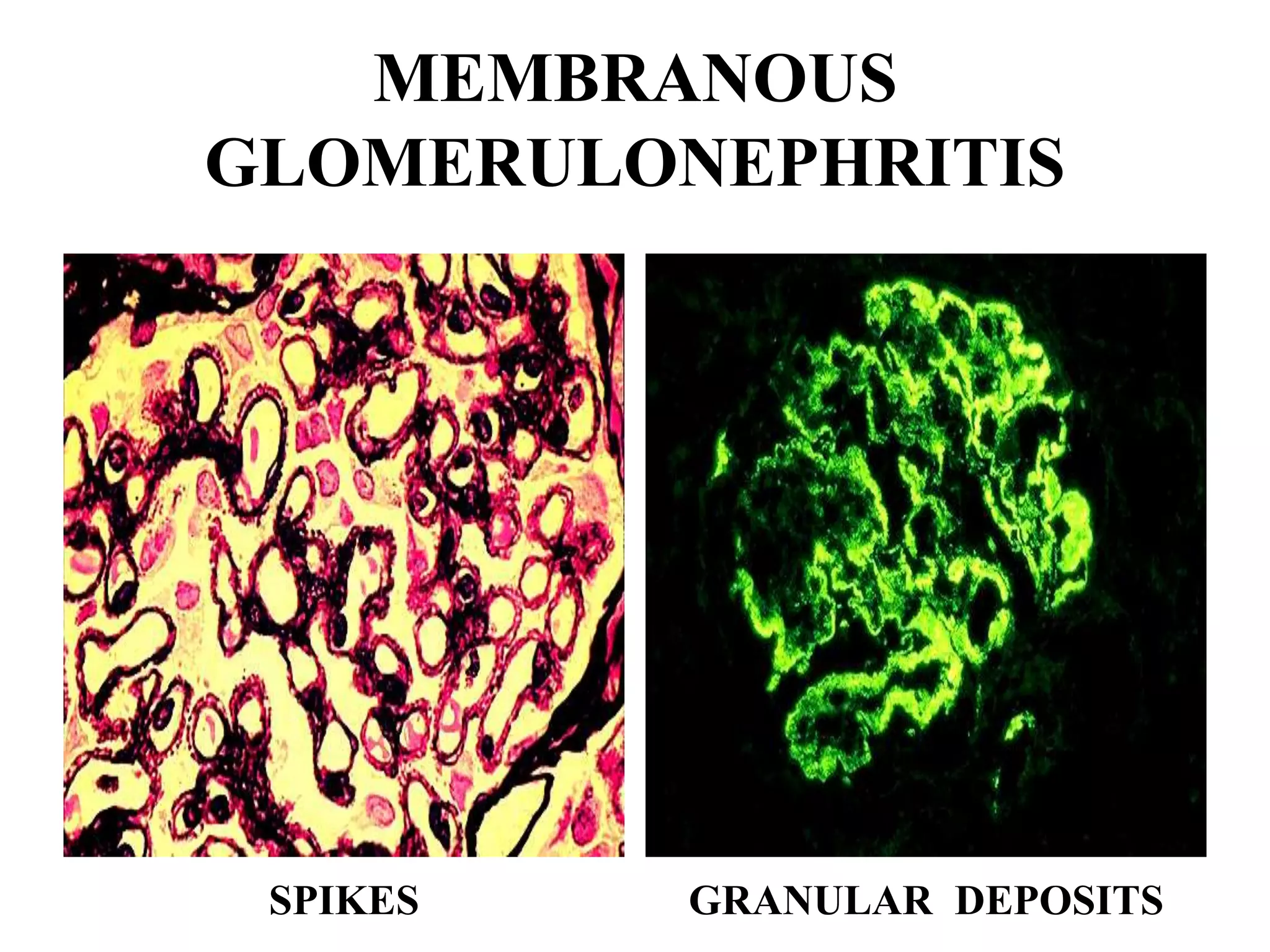



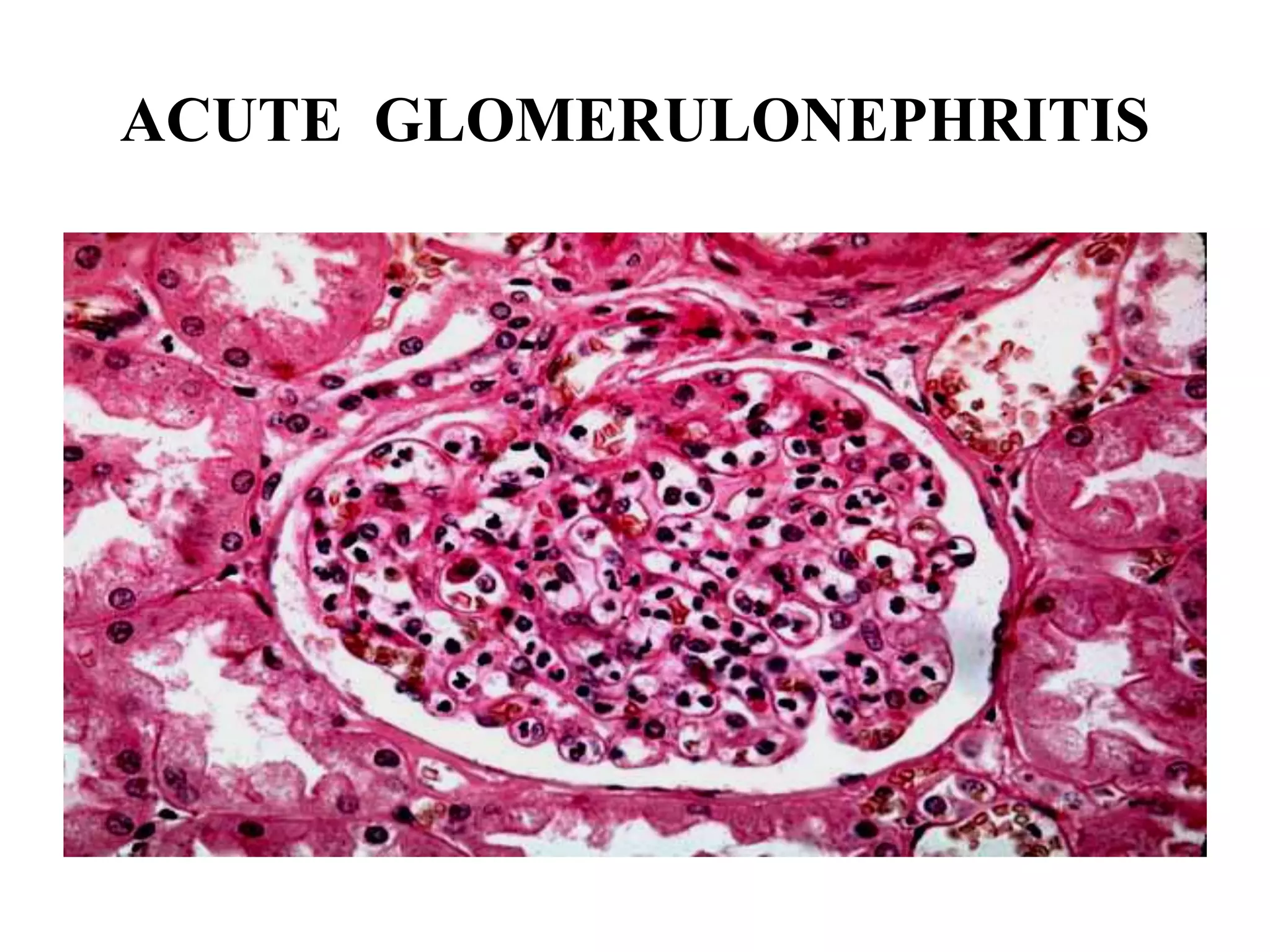

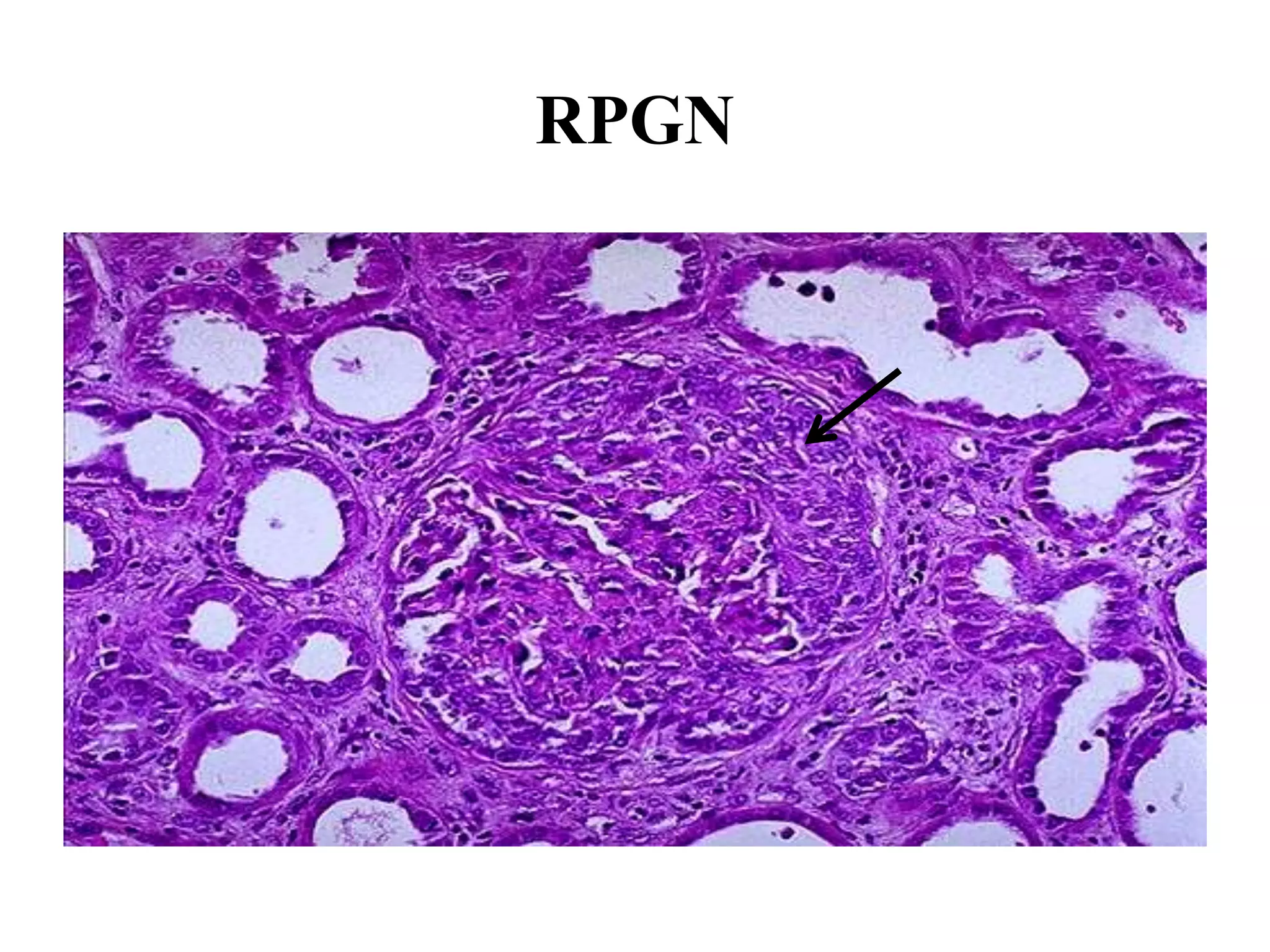


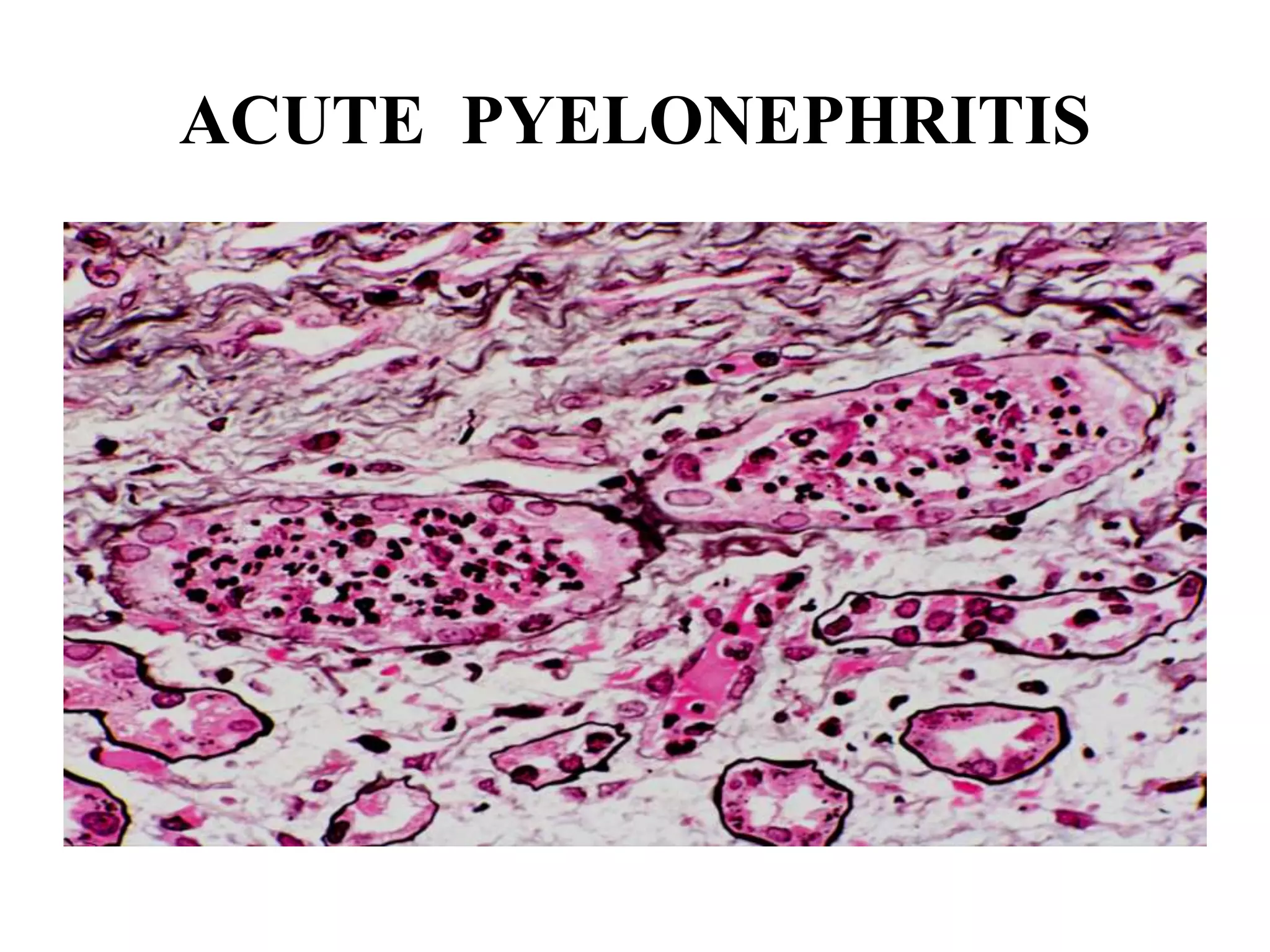
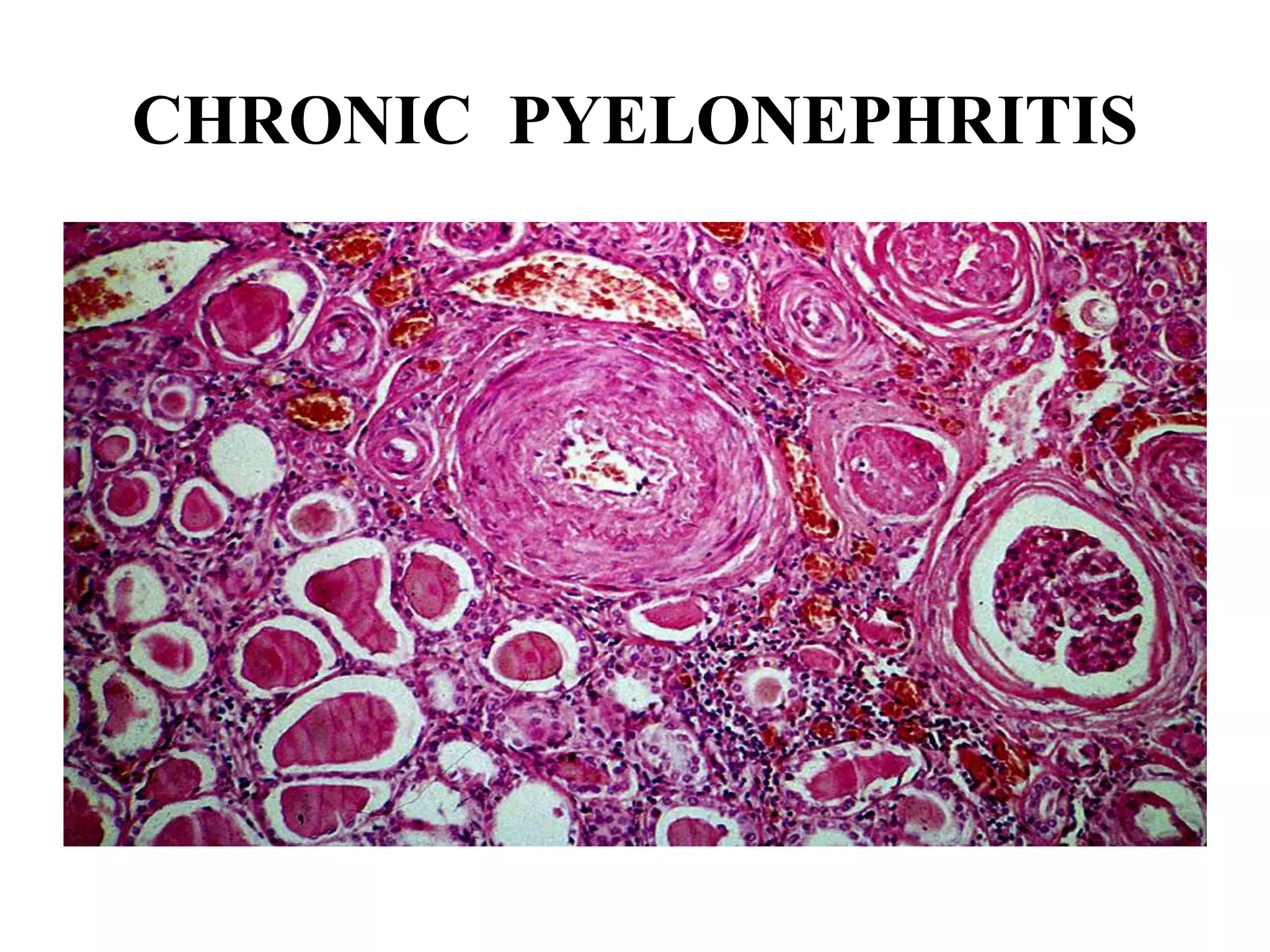








This document discusses laboratory diagnosis of renal diseases. It covers renal function tests like glomerular filtration rate (GFR) and clearance tests which are used to detect early renal impairment. GFR is estimated using creatinine clearance tests or formulas using serum creatinine. Urine analysis and renal biopsy are also used to diagnose and characterize renal diseases by examining features under light and electron microscopy. Renal biopsy can identify conditions affecting the glomeruli, tubules, interstitium or blood vessels. Recent advances include use of genomics and proteomics in renal disease diagnosis and classification.



































































