Downloaded 134 times



![Reference-
1. Renal Function Test (RFT). [Internet]. Available from:
Renal Function Test (RFT) - Physiopedia (physio-pedia.com) [Last accessed: 19 August
2021]
2. Gounden V, Bhatt H, Jialal I. Renal Function Tests. [Updated 2020 Jul 20]. In: StatPearls
[Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK507821/
3. Tests to Measure Kidney Function, Damage and Detect Abnormalities. [Internet].
Available from: Tests to Measure Kidney Function, Damage and Detect Abnormalities |
National Kidney Foundation [Last accessed: 19 August 2021]
4. Estimated Glomerular Filtration Rate (eGFR) . [Internet]. Available from: Estimated
Glomerular Filtration Rate (eGFR) | National Kidney Foundation [Last accessed: 19
August 2021]
5. Renal function tests. [Internet]. Available from: Renal function tests (slideshare.net)
[Last accessed: 19 August 2021]](https://image.slidesharecdn.com/mdaltamashpharmd4thyearrenalfunctiontests-210820090627/85/Renal-Function-Tests-RFT-32-320.jpg)

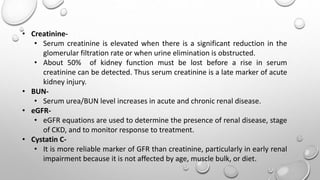
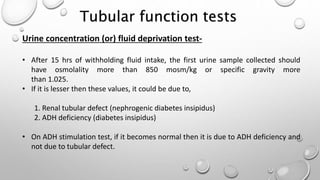
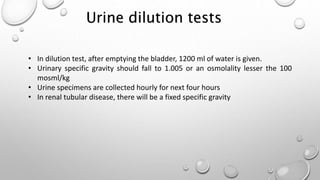
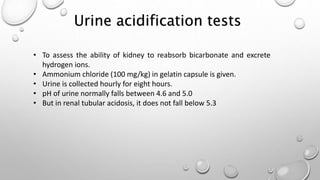
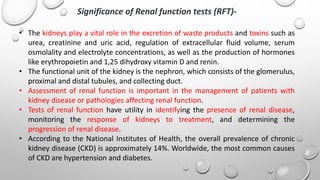
The document discusses renal function tests (RFTs). It provides information on: - The functions of the kidney including homeostasis, excretion, and hormonal functions. - Common RFTs including urine analysis, serum creatinine, BUN, eGFR, and cystatin C. These tests are used to evaluate glomerular filtration rate and detect kidney problems. - Additional details are given on clearance tests using inulin, creatinine and urea to estimate GFR. Urine analysis and tests of tubular function are also summarized.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









