Downloaded 15 times


![ Hyperproteinemia or hyperlipidemia dilutes
out the Na+. [Na+] in the water portion of the
blood is normal.
Glycine solution with TURP.
Treatment is to work up and treat underlying
cause](https://image.slidesharecdn.com/waterandelectrolytesbalancess-200502115917/85/Water-and-electrolytes-balance-ss-50-320.jpg)
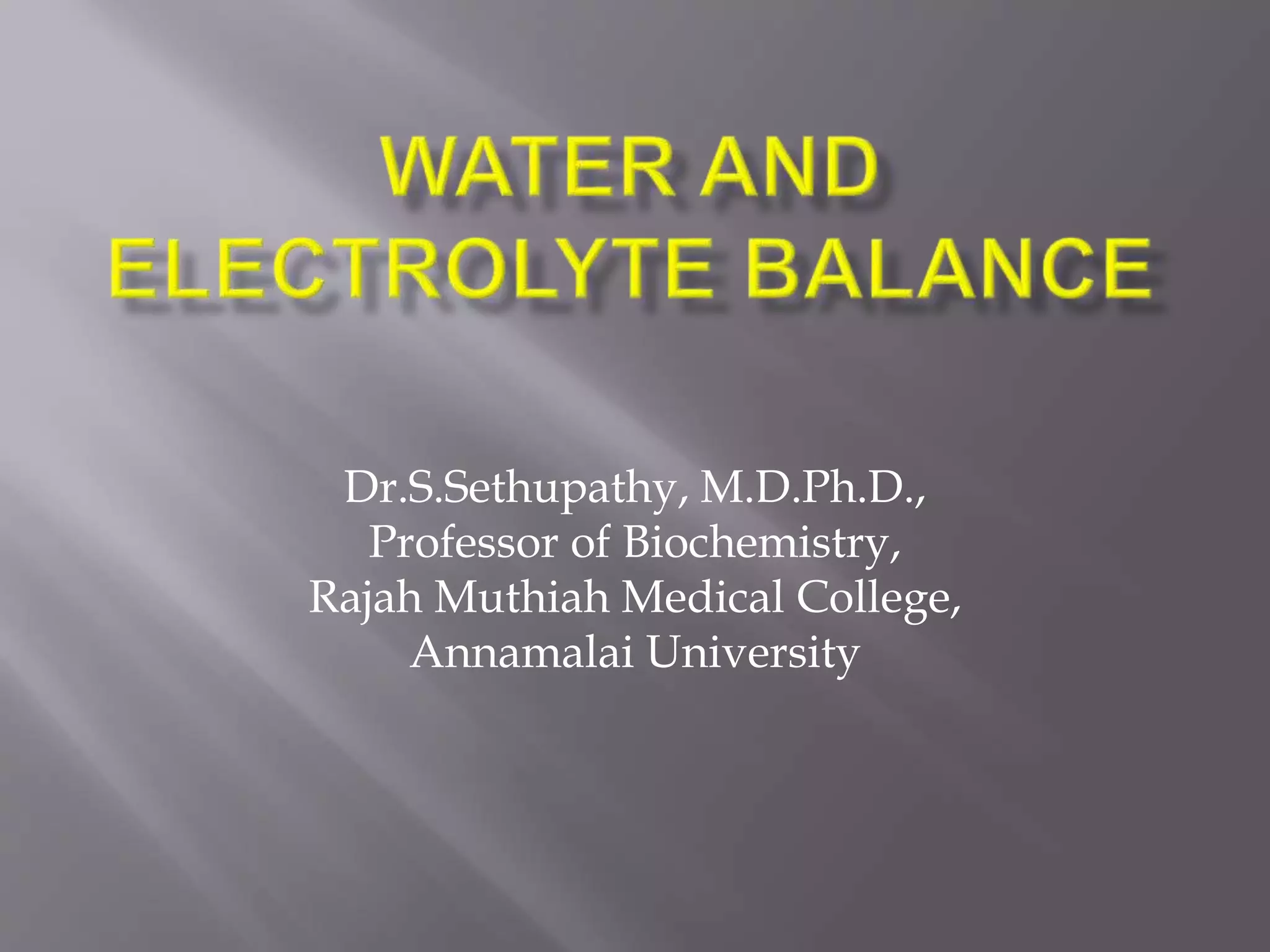
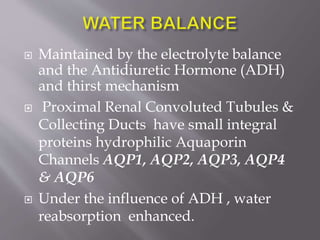
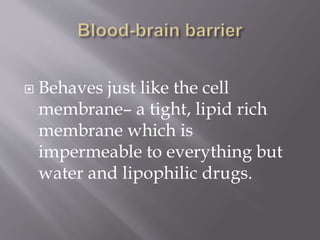
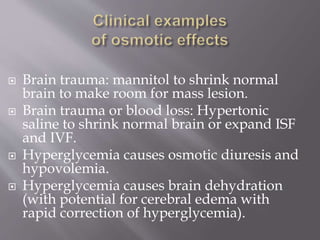
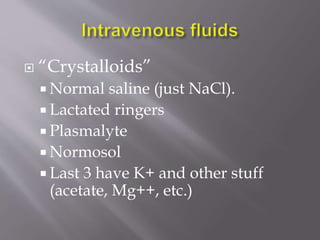
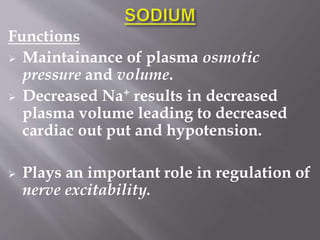
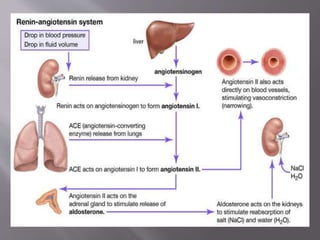
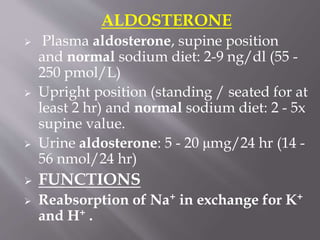
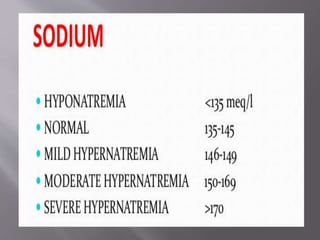
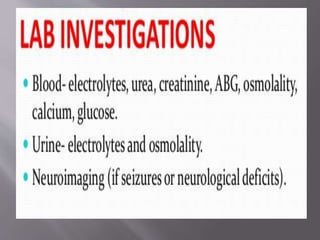
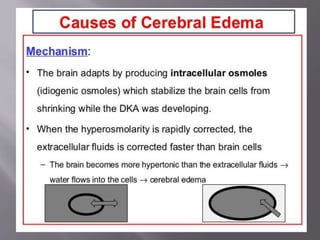
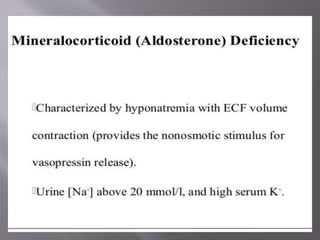
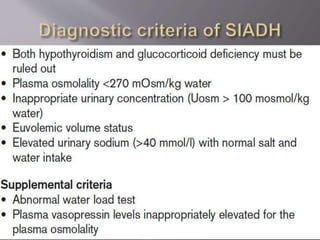
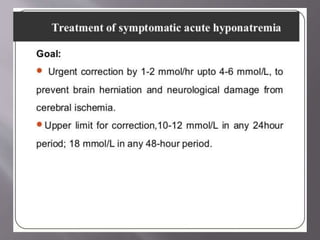
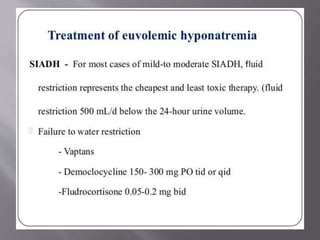
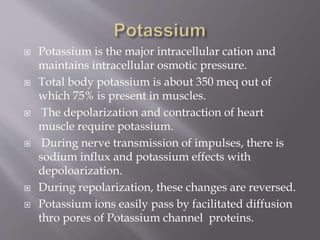
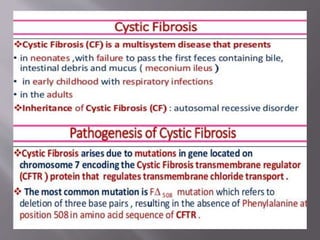
![Protein or lipid
“phase”
[NaCl] = 0
Aqueous “phase”
[NaCl] = 135
Serum
(combined)
[NaCl] = 123
Isotonic hyponatremia (“artifactual”). Protein or lipid
takes up some of the plasma volume. Aqueous “portion”
of plasma has normal [NaCl].
Osmolarity
(tonicity)
normal](https://image.slidesharecdn.com/waterandelectrolytesbalancess-200502115917/85/Water-and-electrolytes-balance-ss-51-320.jpg)
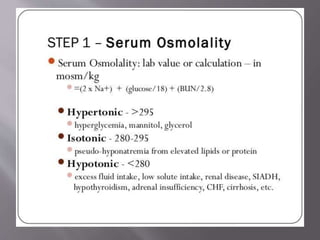
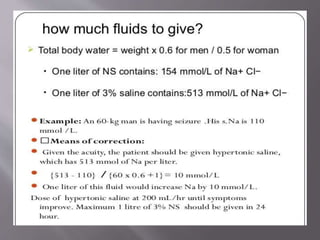
![ Due to hyperglycemia, mannitol or glycerol.
Decreased [Na+] in serum, but osmolality is
high (>290), due to sugar in the blood.
Sugar has “sucked” water out of cells, into the
ECF. Water dilutes Na+.](https://image.slidesharecdn.com/waterandelectrolytesbalancess-200502115917/85/Water-and-electrolytes-balance-ss-52-320.jpg)
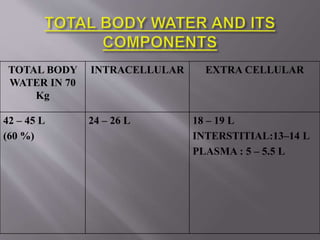
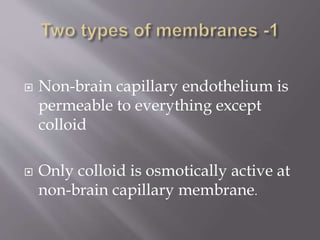
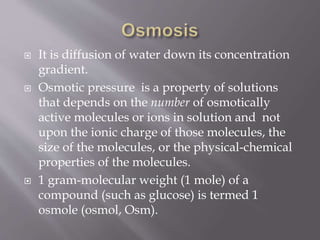
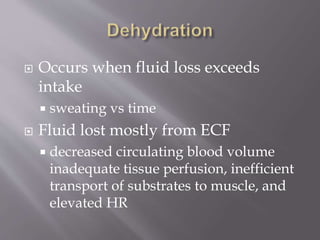
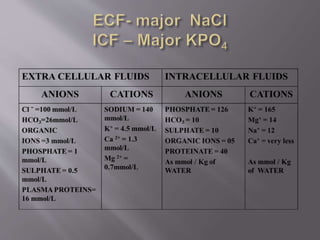
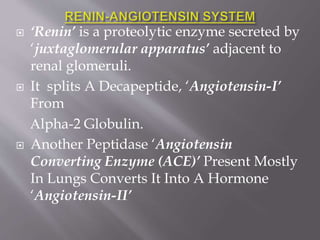
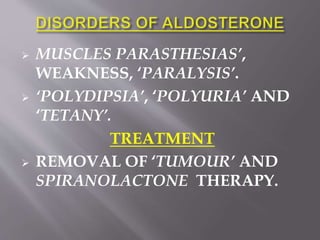
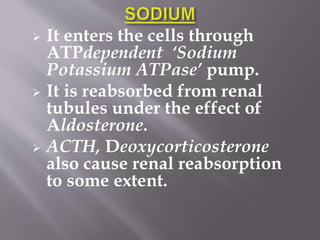
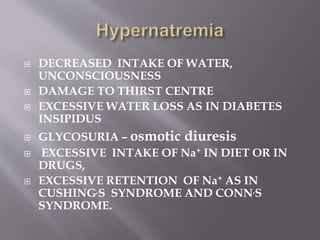
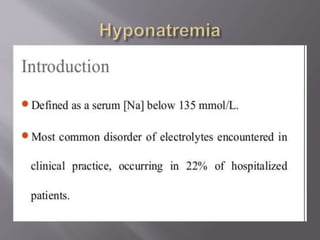
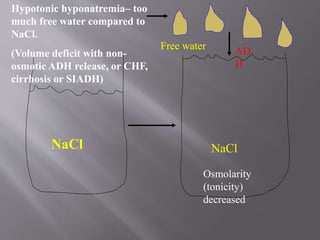
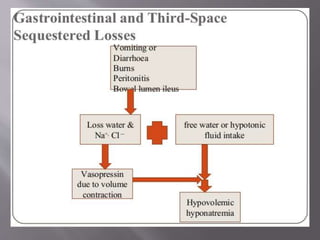
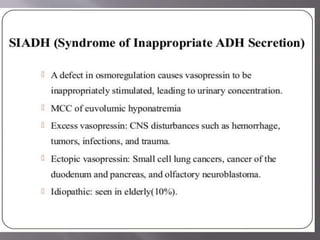
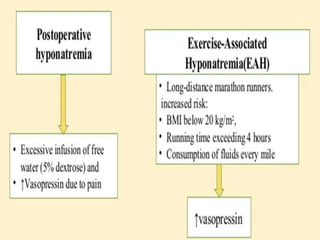
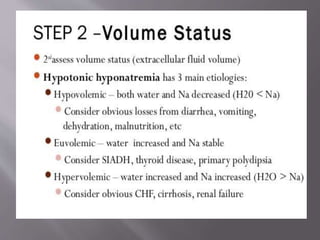
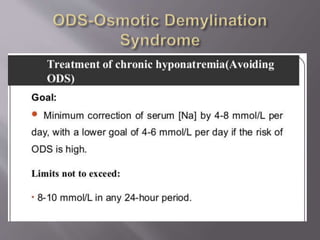
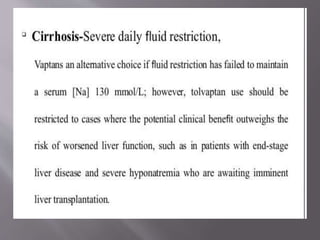
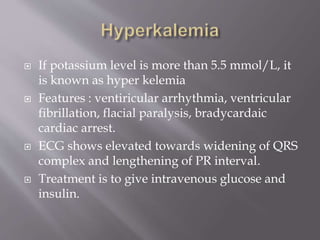
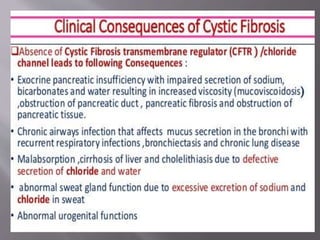
![Water in ICF and
interstitial ECF
[NaCl] =
140 [NaCl] =
123
Glucose,
mannitol,
glycerol
Hypertonic hyponatremia– osmotically active sugar
“draws” water into vascular space, diluting NaCl, but
increasing overall osmolarity (tonicity).
Osmolarity (tonicity)
increased](https://image.slidesharecdn.com/waterandelectrolytesbalancess-200502115917/85/Water-and-electrolytes-balance-ss-53-320.jpg)
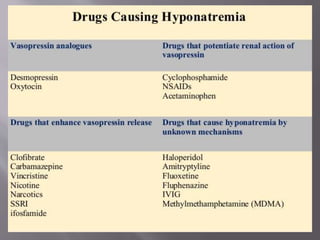


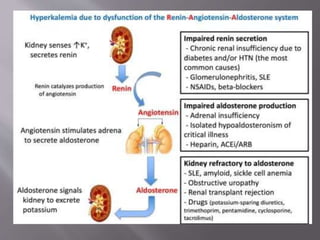
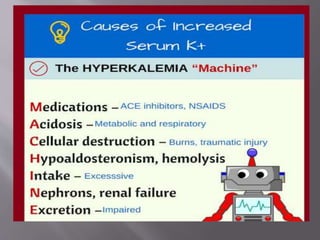


The document discusses the significance of water and electrolyte balance in the human body, accounting for the distribution of total body water and its relation to osmolality. It covers physiological processes, including the roles of hormones such as ADH and aldosterone, effects of various conditions (e.g., dehydration, hyperglycemia), and the impact of electrolyte disturbances on health, particularly sodium and potassium management. Additionally, it outlines clinical signs, disorders related to electrolyte imbalances, and appropriate treatments.

















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





