Downloaded 12 times







































![Example contd…
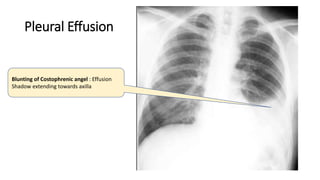
• Probable diagnosis: Lt sided Pleural Efusion
• Expected viva questions:
• What are the different cause of pleural effusion? [TB, empyema, CHF,
cirrhosis, etc]
• What are the clinical features of Pl effusion [Diminished breath sounds,
stony dullness on percussion, diminished VR and VF, etc]
• How to differentiate between an exudate and transudate? [Cell count,
Protein, Gram’s stain, C/s. etc]
• What are the treatment modalities for pleural effusion? [Steroids for TB,
Needle aspirations, Thoracic tube drainage for empyema, etc]](https://image.slidesharecdn.com/xraysforugs-200421023650/85/X-Ray-Reading-for-UGs-71-320.jpg)

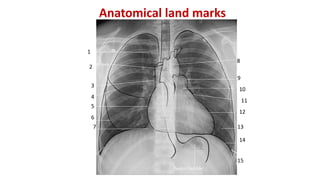
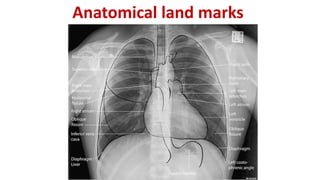
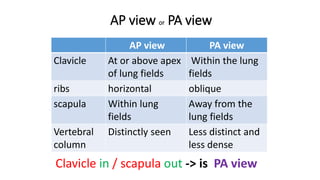
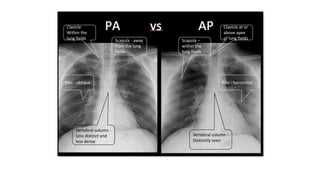
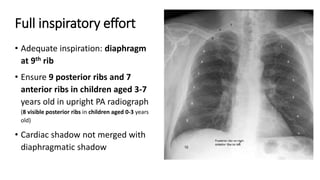
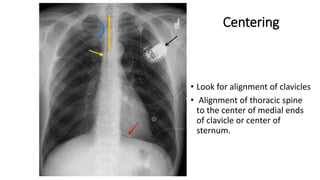
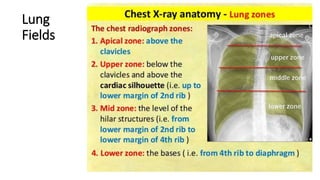
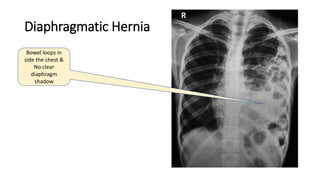
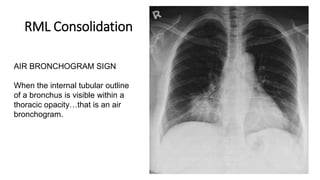
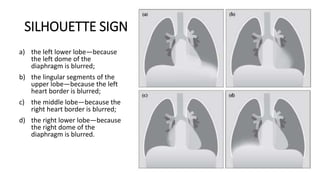
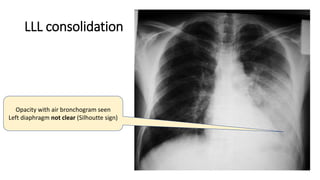
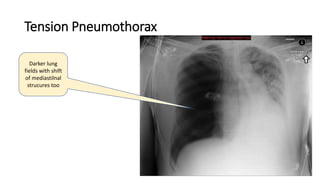
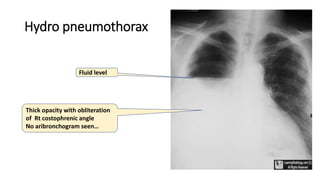
This document provides guidance on reading chest x-rays, including identifying anatomical landmarks, assessing centering and rotation, diagnosing conditions, and common films seen in exams. Key tips include starting with bony landmarks, ensuring full inspiration, and looking for signs like air bronchograms or silhouette signs when diagnosing conditions like pneumonia or effusions. Common conditions covered are pneumothorax, cardiomegaly, and pleural effusions. Examiners are advised to narrate findings and be prepared to discuss related clinical features and treatments.
















![Spleen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/spleen1-171112094140-thumbnail.jpg?width=640&height=640&fit=bounds)






































































