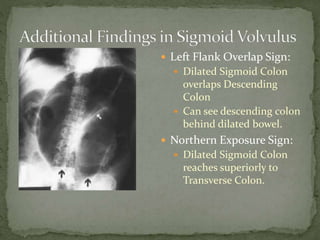
An 80-year-old man presented with acute severe abdominal pain, distention, and constipation. Physical exam revealed a distended abdomen with tenderness worse in the lower left quadrant. Imaging showed signs of sigmoid volvulus including the coffee bean sign and left flank overlap sign. Treatment included decompression, IV fluids, analgesics, and surgical consultation given the risk of complications from the sigmoid volvulus like ischemia or perforation.