Downloaded 171 times


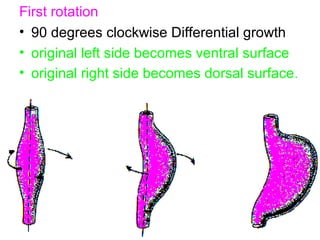
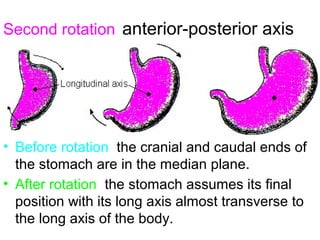
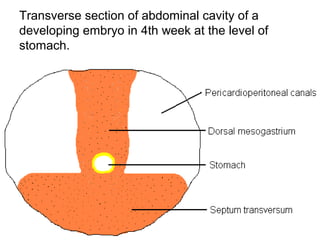
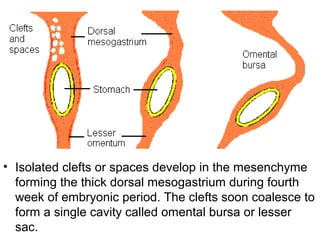
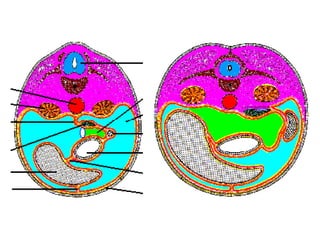
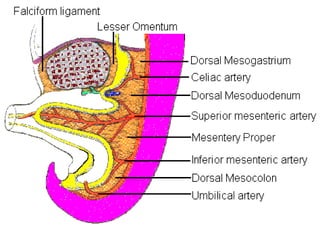
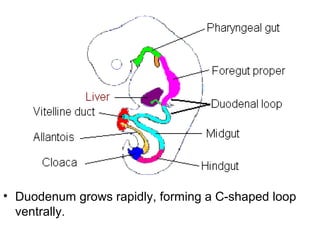
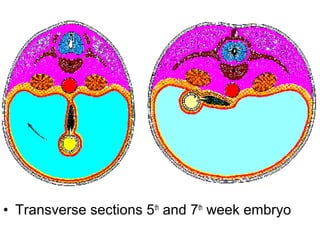

The stomach develops from the foregut as a simple tubular structure that enlarges dorsally through differential growth. It rotates along two axes, determining its final position in the left hypochondrium. The dorsal mesogastrium suspends the stomach and later forms the greater omentum. The duodenum develops from the foregut and midgut, forming a C-shaped loop that rotates to the right as the stomach rotates left. Both become retroperitoneal as their mesenteries fuse with the posterior abdominal wall.











































































































