Downloaded 96 times



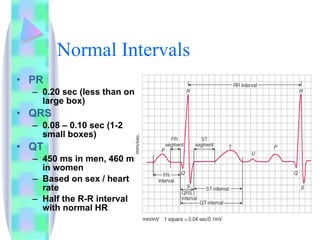
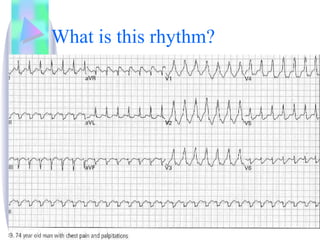
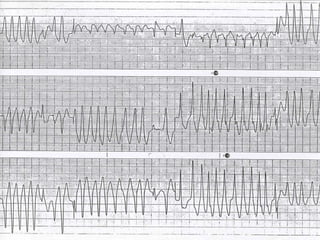
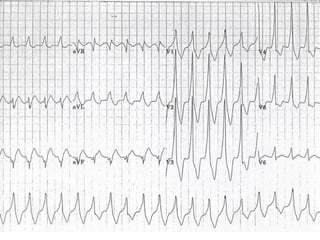
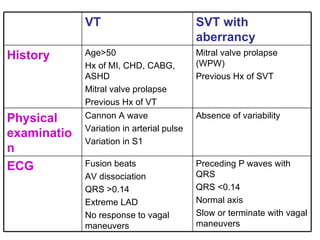
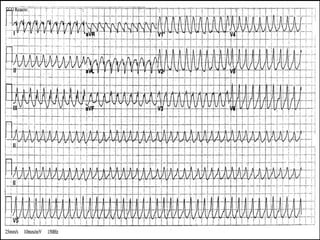
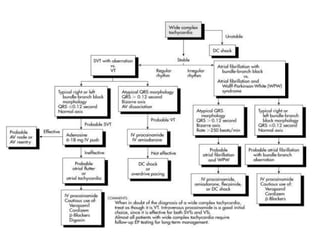

1. Wide complex tachycardia (WCT) refers to tachycardias with a heart rate over 100 beats per minute and a QRS duration greater than 0.12 seconds. 2. WCT can be caused by irregular rhythms like atrial fibrillation or regular rhythms like supraventricular tachycardia with aberrant conduction or ventricular tachycardia. 3. Management depends on hemodynamic stability and rhythm characteristics - synchronized cardioversion is first-line for unstable patients, while antiarrhythmic drugs or pacing are used for stable patients depending on the underlying rhythm.