Download as PDF, PPTX

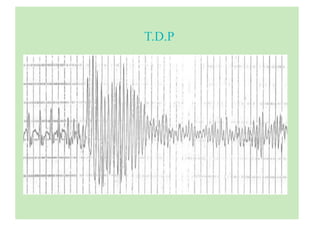
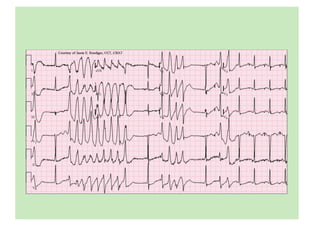
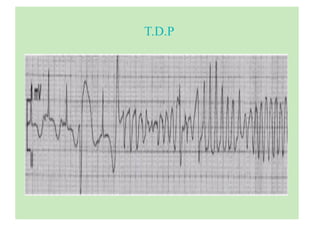
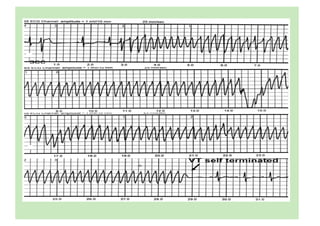
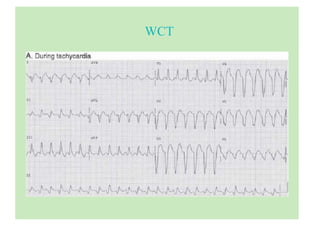
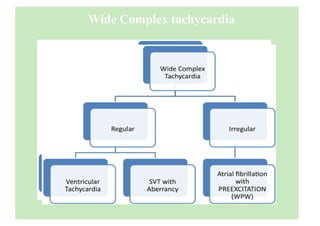
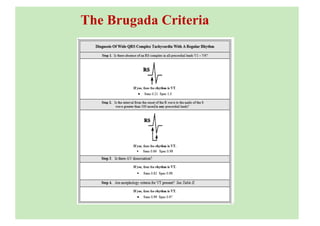
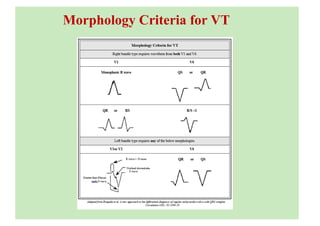
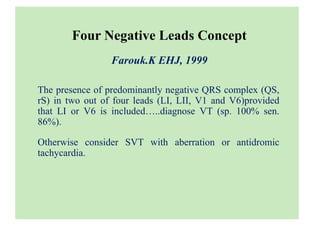
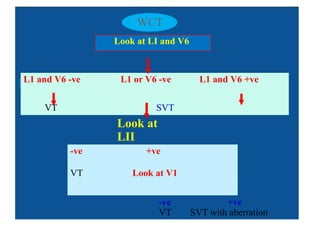
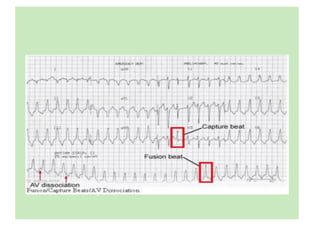
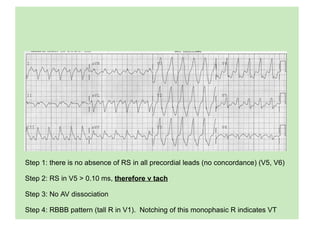
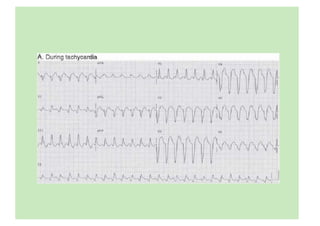
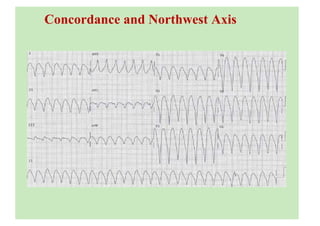
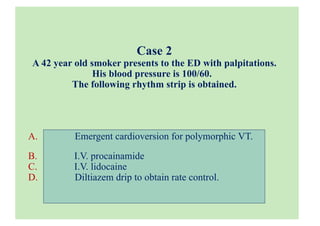
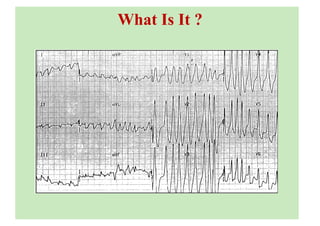



The document discusses ECG interpretations for various cardiac arrhythmias, particularly for intensive care scenarios involving ventricular tachycardia (VT), atrial fibrillation, and Wolff-Parkinson-White syndrome. It highlights essential diagnostic criteria, treatment options, and case studies for understanding and managing these conditions in patients with differing presentations and histories. Additionally, it outlines important rules and recommendations for handling arrhythmia cases efficiently.





























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








