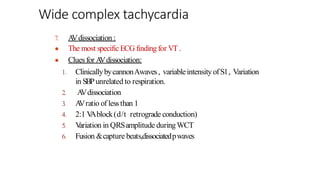
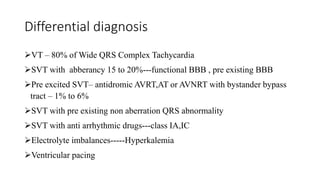
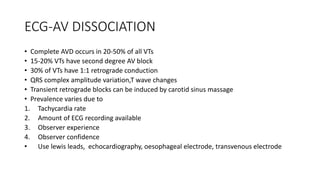
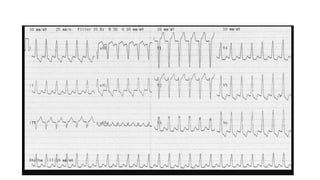
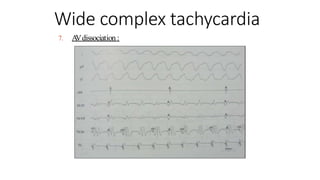
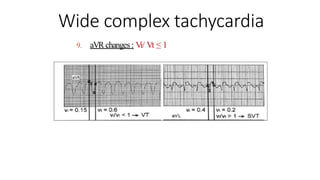
This document discusses wide complex tachycardia (WCT), which is defined as a heart rate over 100 beats per minute with a QRS duration greater than 120 ms. The main causes of WCT are ventricular tachycardia (VT), supraventricular tachycardia (SVT) with abnormal conduction, and ventricular pacing rhythms. The document outlines various diagnostic features on ECG that can help differentiate VT from SVT such as QRS axis, morphology, presence of AV dissociation, and criteria involving leads aVR and lead II R-wave peak time. Algorithms combining multiple ECG criteria can identify VT with high sensitivity and specificity. History, physical exam findings, and response to treatments may also provide





























































![Wide complex tachycardia
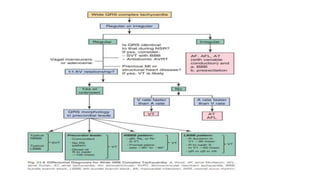
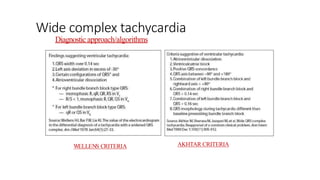
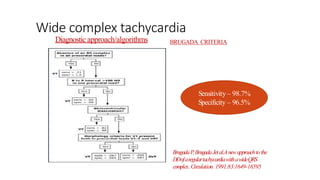
Diagnostic approach/algorithms
Sen.10%
Spe.100%
Sen.48%
Spe.98%
Sen.89%
Spe.89%
Sen.95%
Spe.80%
The sensitivity [95.7 vs.
88.2, P< 0.001]and NPV
[83.5%vs. 65.3% for VT
diagnosis ofthe new
algorithmwere superior to
those of the Brugada criteria
Application of anewalgorithmin the DD
of wideQRScomplextachycardia Andra´s
V
ereckei et al . EHJ2007.](https://image.slidesharecdn.com/finalpptwidecomplextachycardia-230807075938-18e84faa/85/wide-complex-tachycardia-pptx-79-320.jpg)