Downloaded 193 times

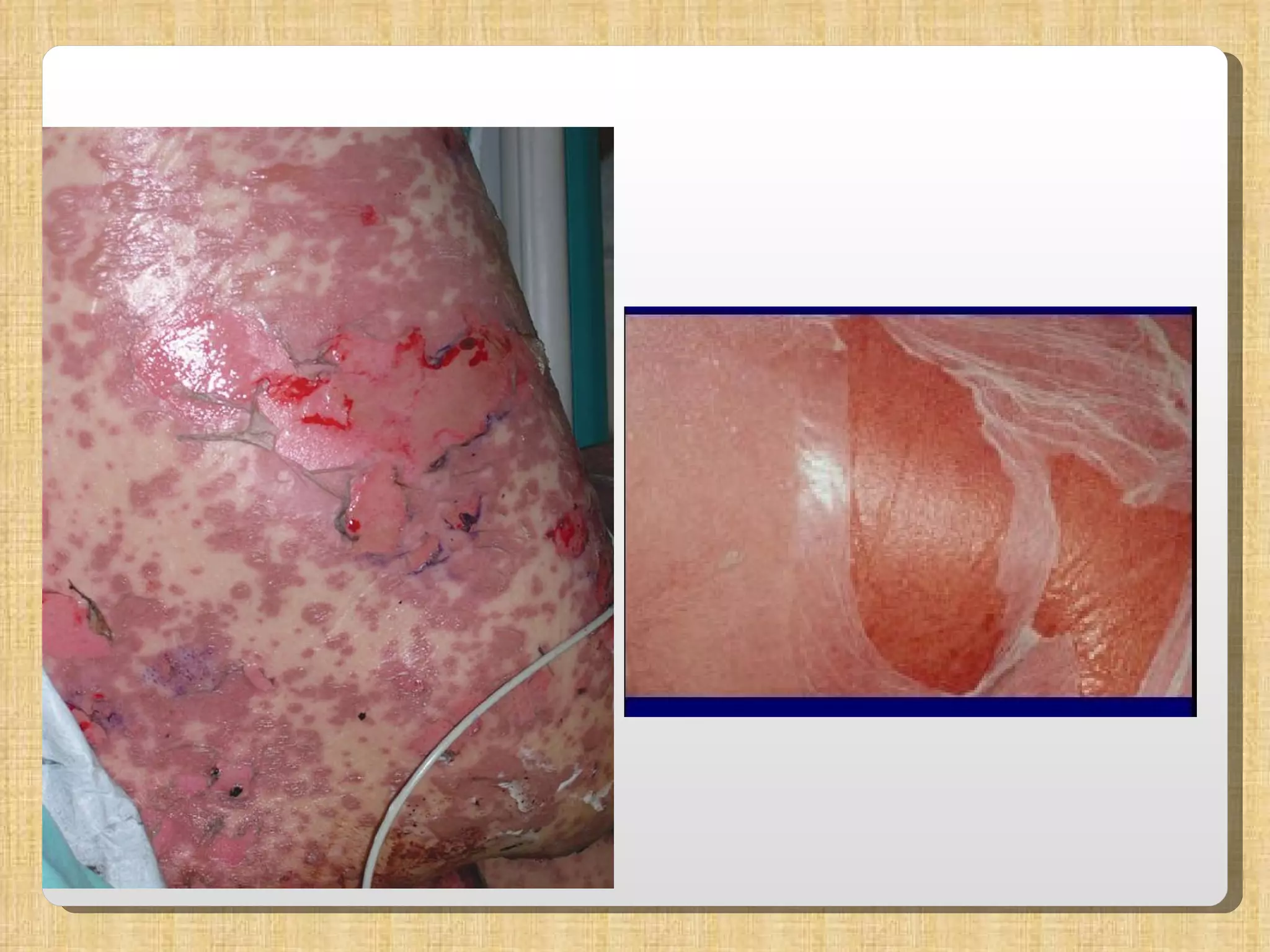

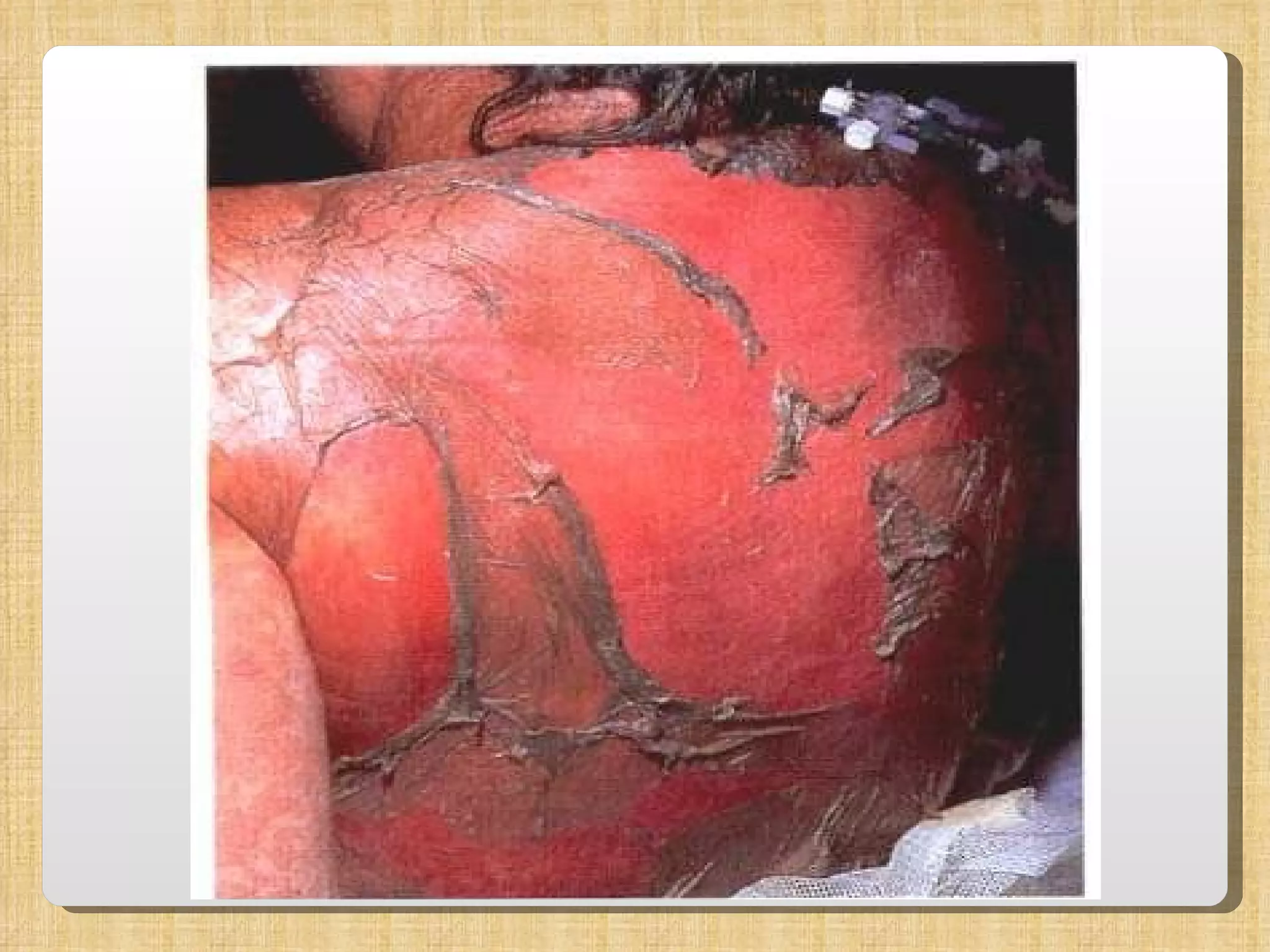





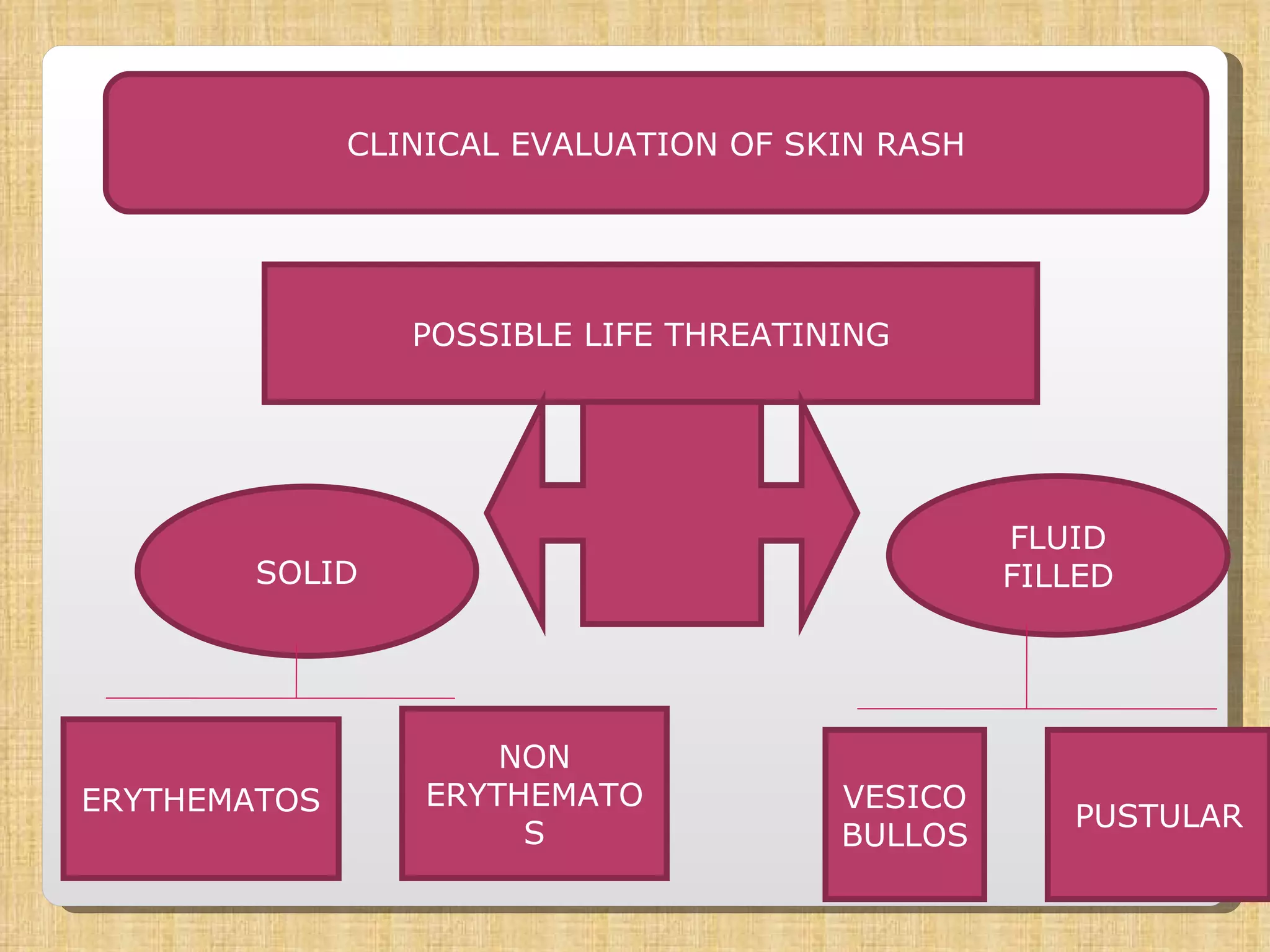



1. The document discusses the evaluation and management of patients presenting with rashes, focusing on acute skin failure. It outlines the key components of obtaining a history, physical examination of different rash morphologies, and challenges in diagnosing conditions like Steven-Johnson syndrome. 2. Management requires a multidisciplinary approach across nursing, monitoring of hemodynamics and nutrition, and topical therapies. Poor prognostic factors include older age, larger surface area involvement, and underlying conditions. 3. Treatment recommendations are made for conditions like Steven-Johnson syndrome, with glucocorticoids suggested for adults within 24-48 hours but not for toxic epidermal necrolysis due to risk of sepsis. Intravenous immun



































































