Downloaded 364 times

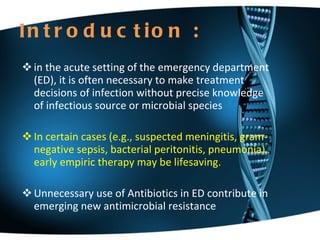
















![Presence of comorbidities, - chronic heart, lung,liver, or renal disease - diabetes mellitus; ---alcoholism; malignancies; asplenia; immunosuppressing use of immunosuppressing drugs; use of antimicrobials within the previous 3 months (in which case an alternative from a different class should be selected) A respiratory fluoroquinolone (moxifloxacin, gemifloxacin,or levofloxacin (level I evidence) A b-lactam plus a macrolide (strong recommendation (level I evidence) alternatives include ceftriaxone, cefpodoxime, and cefuroxime [500 mg 2 times daily]; doxycycline [level II evidence]](https://image.slidesharecdn.com/abined-101221111555-phpapp02/85/Antibiotic-in-ED-20-320.jpg)


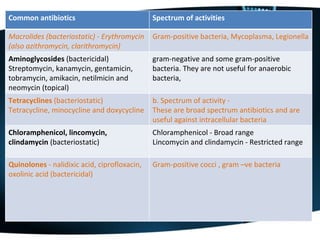
![Empiric Therapy—immunocompetent Age: Preterm to <1 mo Group B strep 49%, E. coli 18%, listeria 7%, AMP + cefotaxime AMP + gentamicin Age: 1 mo– 50 yrs S. pneumo, meningococci, H. influenzae now very rare, listeria unlikely if young & immuno-competent (add ampicillin if suspect listeria: 2 gm IV q4h) Adult dosage: [( Cefotaxime 2 gm IV q4–6h OR ceftriaxone 2 gm IV q12h)] + ( dexamethasone) + Vanco [( MER 2 gm IV q8h) (Peds: 40 mg/kg IV q8h)] + IV dexamethasone + vanco](https://image.slidesharecdn.com/abined-101221111555-phpapp02/85/Antibiotic-in-ED-23-320.jpg)





















This document discusses the appropriate use of antibiotics in emergency settings. It begins with an introduction on the need for early empiric antibiotic therapy in some infections. It then outlines the indications and spectrum of activity of commonly used antibiotics for conditions like UTI, meningitis, pneumonia, and soft tissue infections. It emphasizes that delays in administering antibiotics in conditions like meningitis and sepsis are associated with worse outcomes.



































































