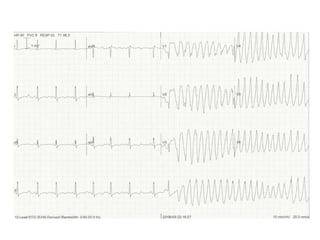
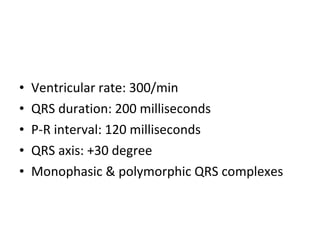
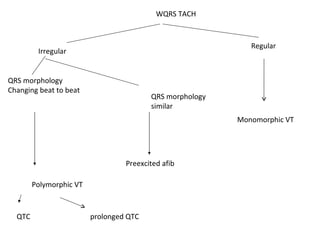
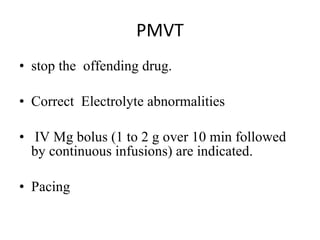
A 46-year-old woman presented with palpitations and breathlessness. Her ECG showed a wide QRS tachycardia at 300 beats per minute with a changing QRS morphology. This is consistent with polymorphic ventricular tachycardia. Intravenous magnesium is the drug of choice for polymorphic VT related to digitalis toxicity or hypomagnesemia. For stable monomorphic VT, intravenous beta blockers are preferred as the initial treatment. Refractory VT may require additional treatments such as amiodarone, overdrive pacing, or an intra-aortic balloon pump.

































![Cardiccccac Arrhythmias [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cardiacarrhythmiasautosaved-241108153215-72acce97-thumbnail.jpg?width=640&height=640&fit=bounds)























































