Downloaded 297 times
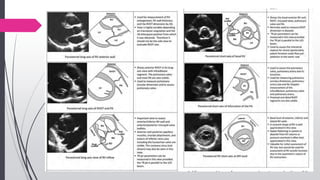


![Estimation of RA pressure from IVC
diameter
Variable Normal (0-5
[3] mm Hg)
Normal (0-5 [3] mm Hg)
Intermediate (5-10 [8]
mm Hg)
High (15mm)
IVC diameter ≤ 2.1 cm ≤ 2.1 cm >2.1 cm >2.1 cm
Collapse with
sniff
>50% <50% >50% <50%
Secondary
indices of
elevated RA
pressure
Restrictive filling
Tricuspid E/E0 > 6
Diastolic flow
predominance in hepatic
veins (systolic filling
fraction < 55%)
Ref: ASE 2010](https://image.slidesharecdn.com/echoassessmentofrvfunction-190104172505/85/Echo-assessment-of-RV-function-38-320.jpg)


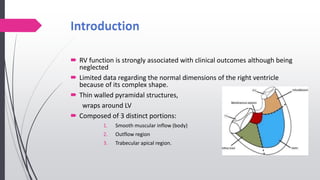
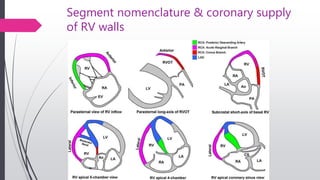
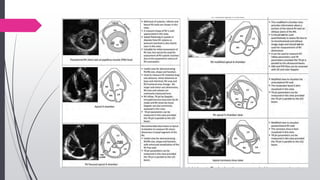
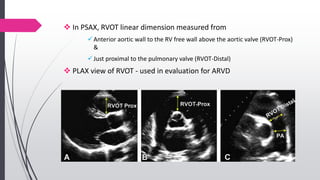
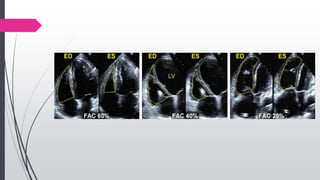
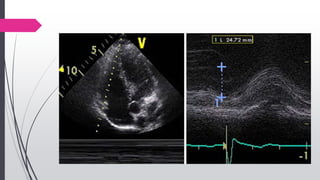
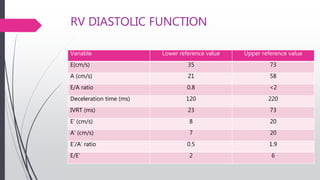
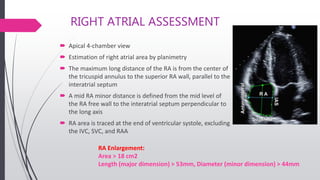
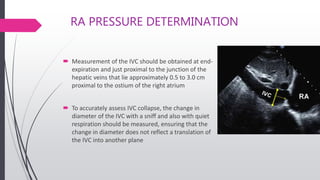
The document provides an overview of right ventricular assessment using echocardiography. It discusses normal RV anatomy, segmental nomenclature, and coronary supply. Key metrics for evaluating RV size, wall thickness, function, and pressures are outlined. Normal values and technical aspects of measuring RV dimensions, area/fractional area change, tricuspid annular plane systolic excursion, myocardial velocity, and diastolic function are summarized. Hemodynamic assessment of pulmonary pressures is also reviewed.



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




