Downloaded 177 times













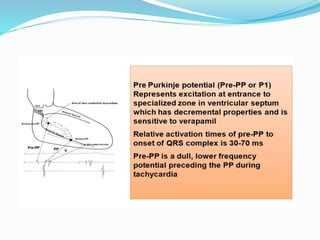
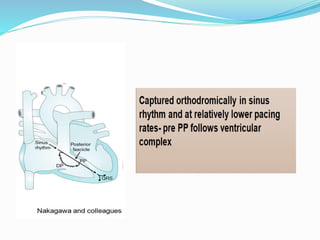

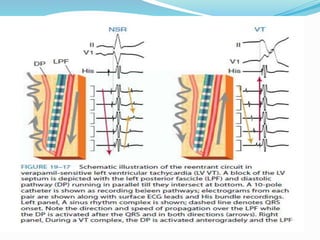


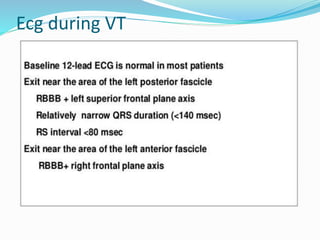
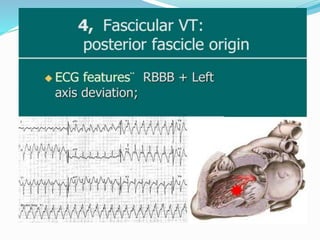
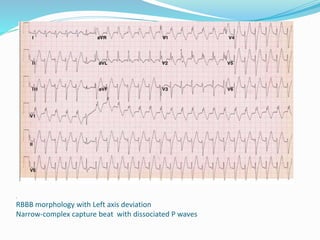

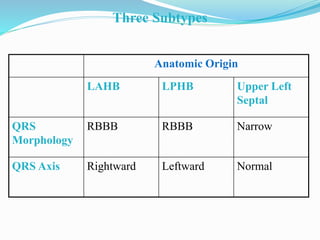
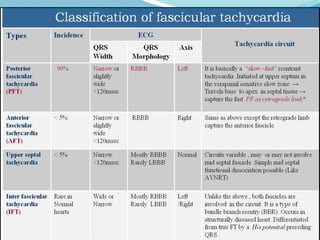



Fascicular ventricular tachycardia is a type of ventricular tachycardia that originates in the Purkinje fibers near the fascicles of the left bundle branch. It typically presents in young males as palpitations or dizziness. The electrocardiogram shows a narrow QRS complex tachycardia with right bundle branch block morphology that is sensitive to verapamil. The reentrant circuit involves abnormal Purkinje fibers as the slow pathway and the left posterior fascicle as the fast pathway. Radiofrequency ablation targeting Purkinje potentials in the left ventricular septum is effective for treatment.










































![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)











































