Downloaded 202 times

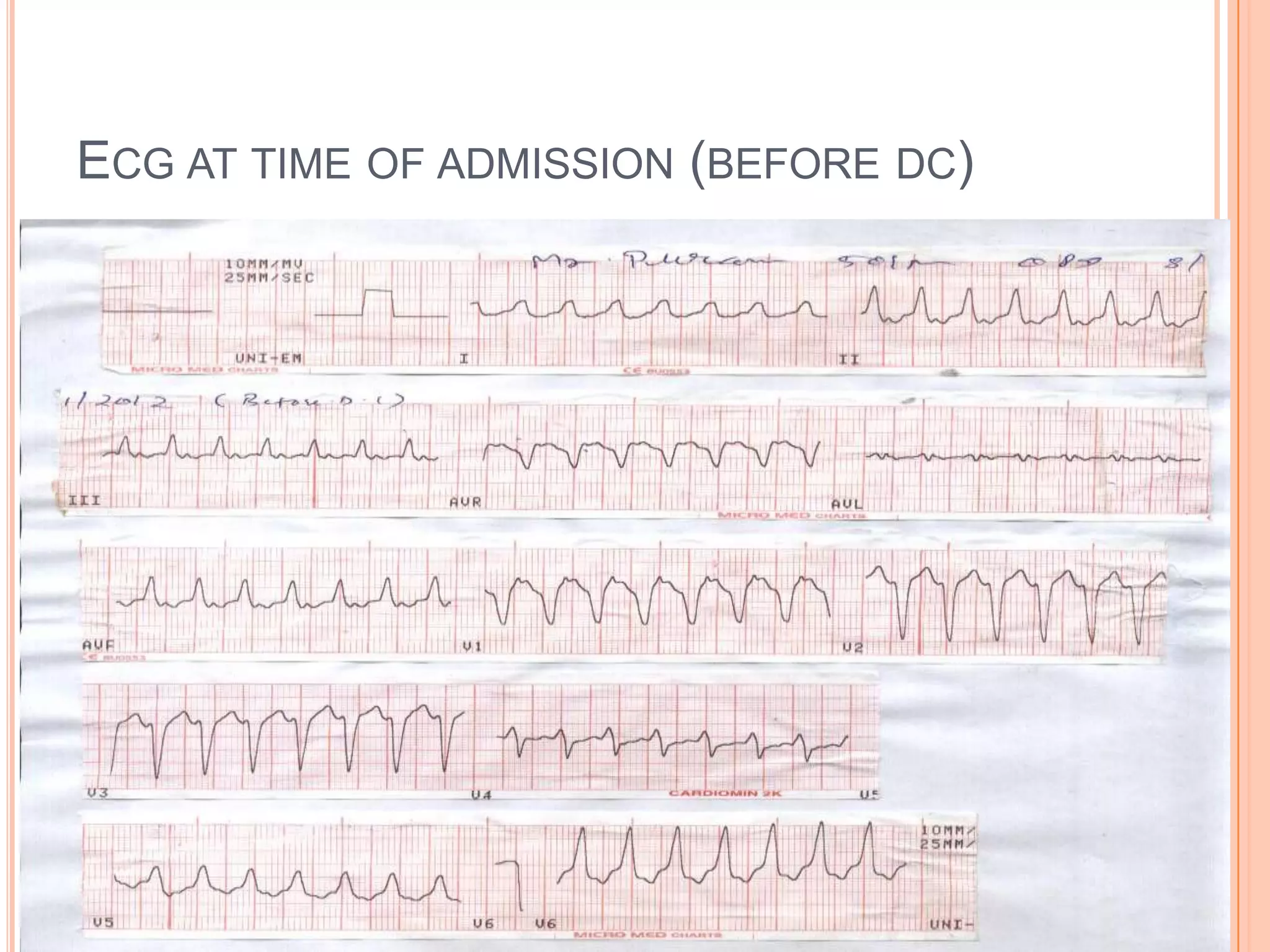



















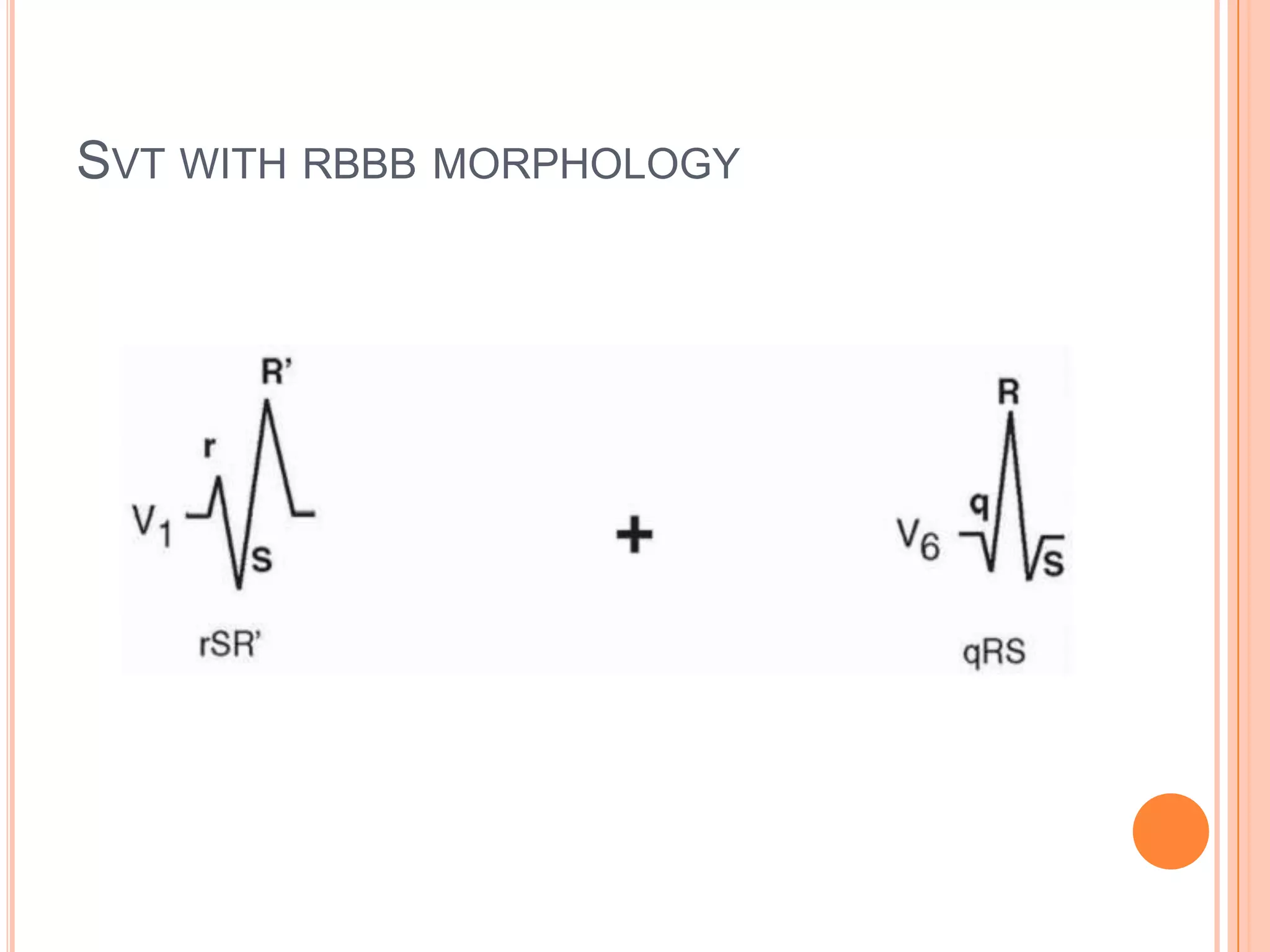






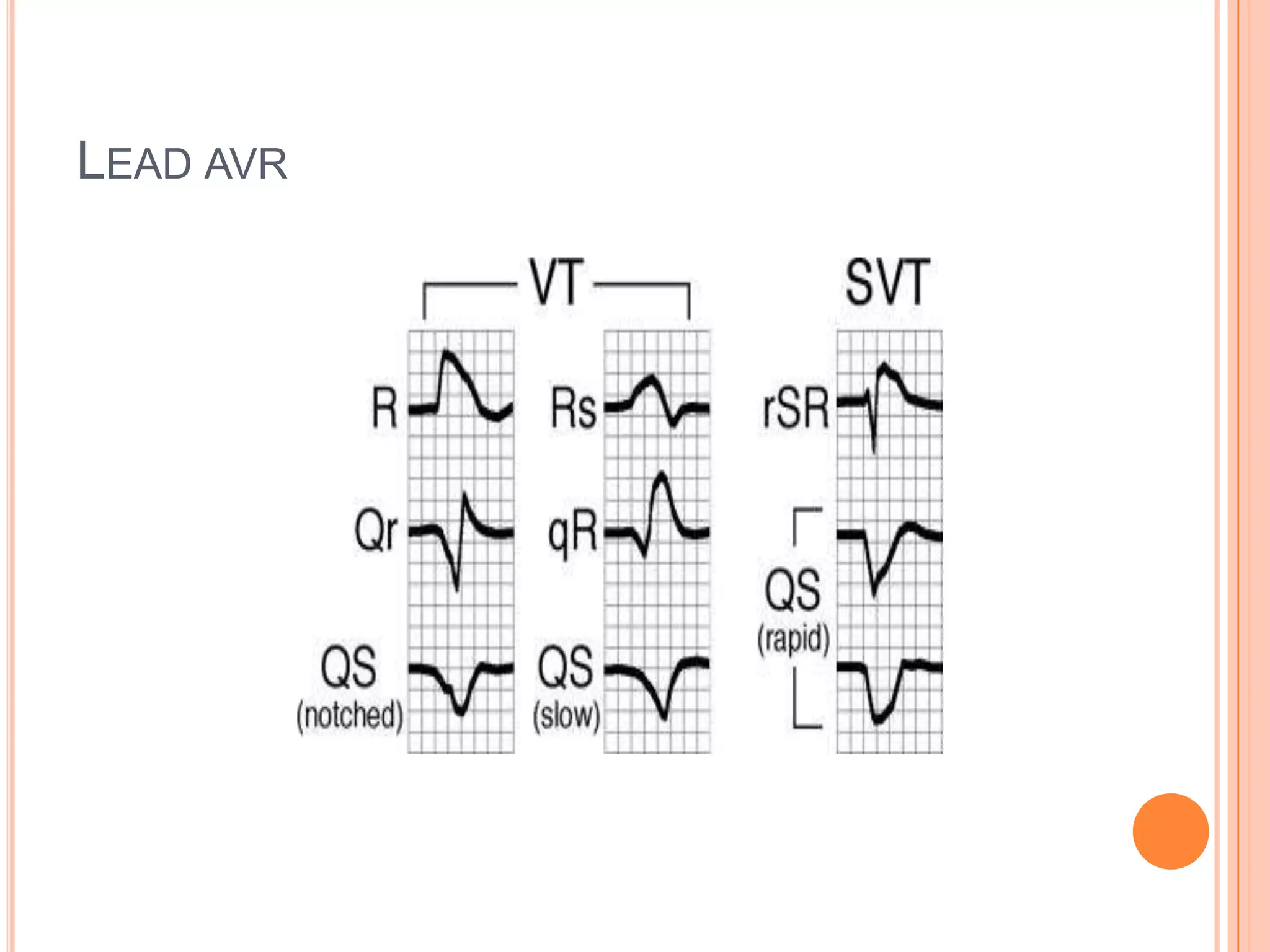







This document summarizes an ECG of a 55-year-old male patient presenting with palpitations. The initial ECG shows a wide complex tachycardia. Differential diagnoses include ventricular tachycardia or supraventricular tachycardia with aberrancy. ECG features favoring ventricular tachycardia over supraventricular tachycardia are discussed, including Brugada criteria and the lead AVR algorithm. Analysis of the patient's ECG determines the rhythm is ventricular tachycardia with left bundle branch block morphology based on his history of myocardial infarction.




















































































