Downloaded 164 times


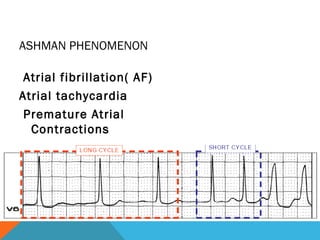
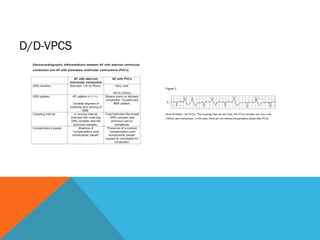

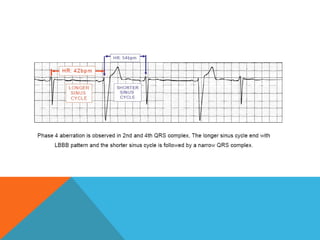

This document defines and describes different types of aberrancy in ventricular conduction. It discusses mechanisms of aberrancy including premature arrival of supraventricular impulses and refractoriness of conducting tissue. Types of aberrancy include type A from fascicular refractoriness, type B from anomalous activation, and type C from paradoxical critical rate. Ashman phenomenon and acceleration/bradycardia-dependent aberrancy are also summarized.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













