Downloaded 313 times

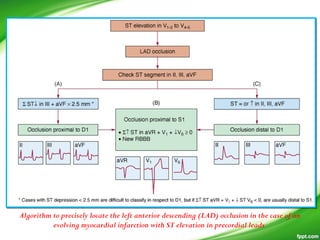
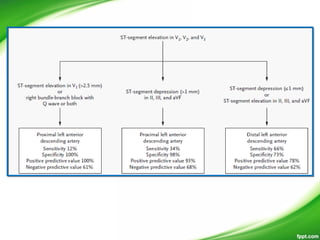
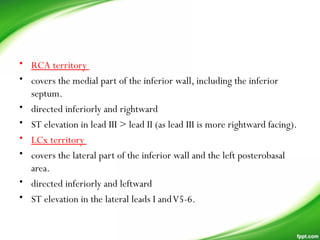
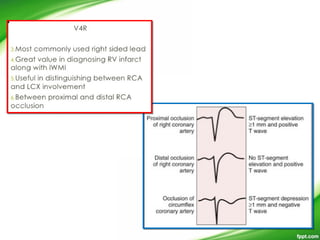
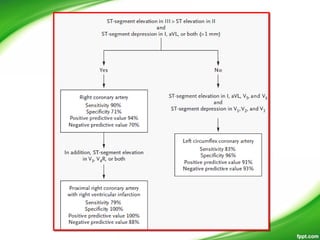
![Algorithm to predict the culprit artery (right coronary
artery [RCA] vs left circumflex artery [LCX]) in case of
evolving myocardial infarction with ST elevation in inferior
leads](https://image.slidesharecdn.com/miecglocalisation-180722060341/85/Myocardial-infarction-MI-ecg-localisation-81-320.jpg)
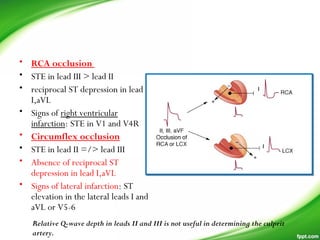
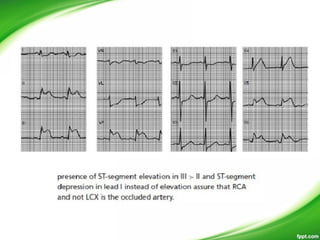
![Algorithm to predict the culprit artery (right coronary
artery [RCA] vs left circumflex artery [LCX]) in case of
evolving myocardial infarction with ST elevation in inferior
leads](https://image.slidesharecdn.com/miecglocalisation-180722060341/85/Myocardial-infarction-MI-ecg-localisation-82-320.jpg)
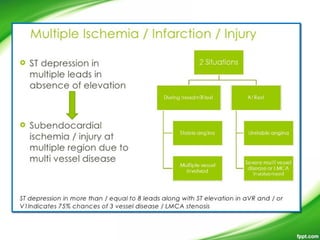
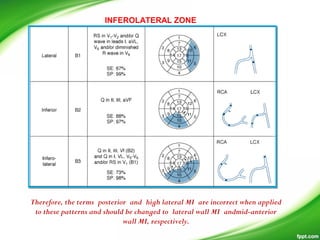
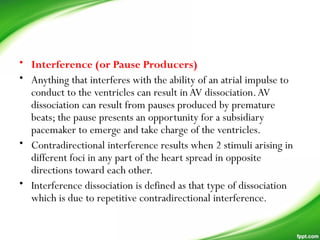

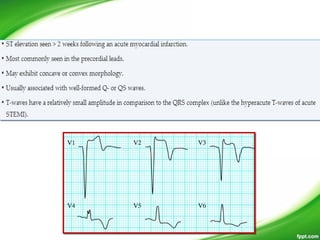
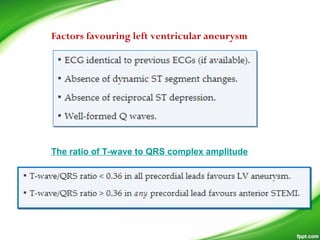
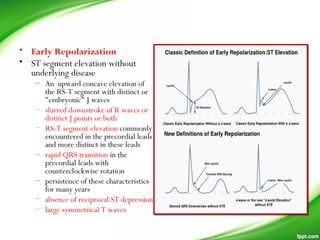
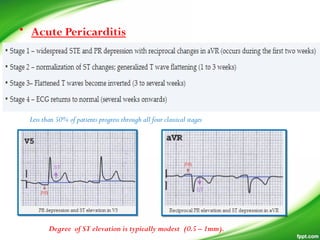
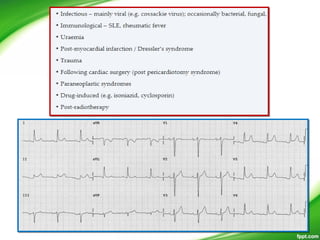
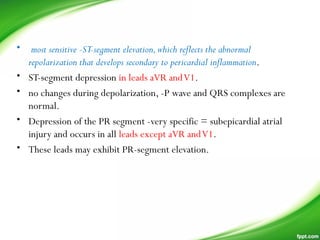
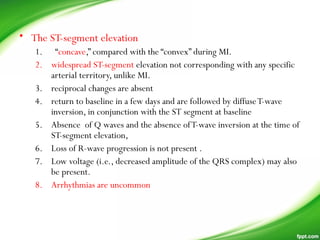
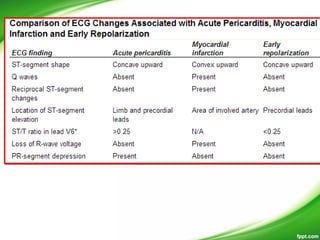
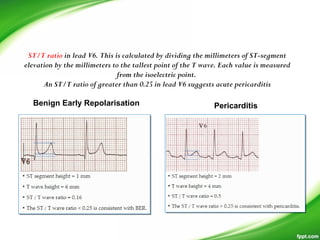
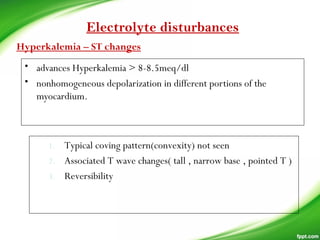
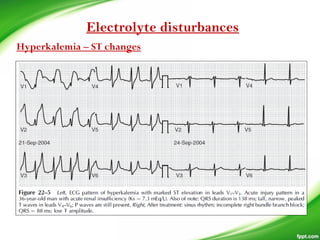
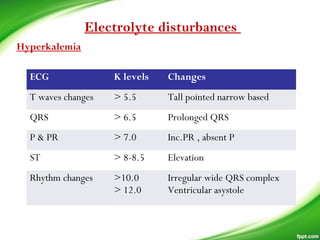
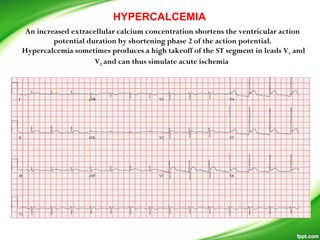
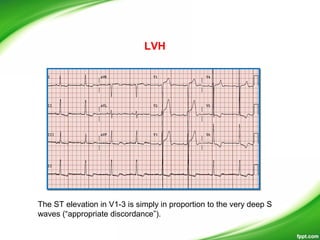
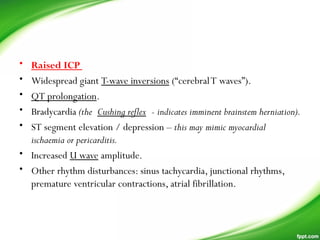
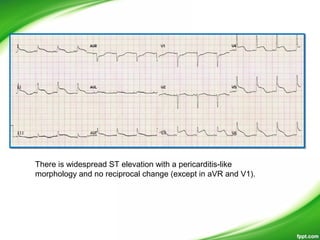
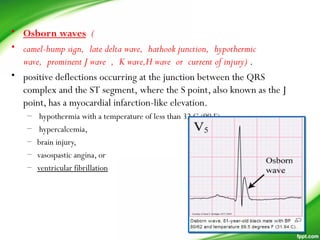
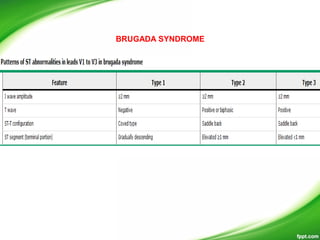
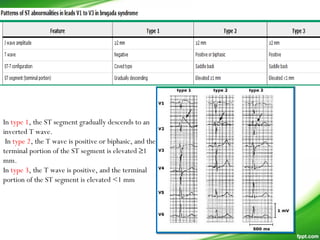
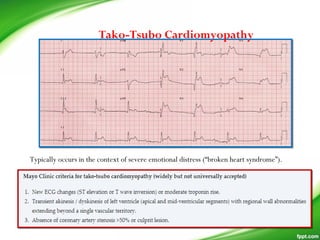
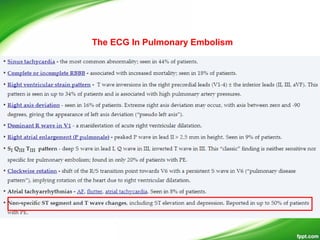
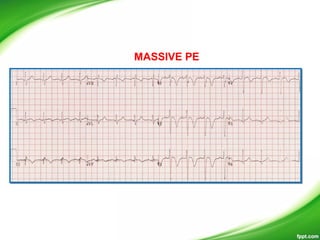
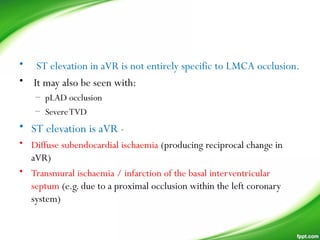
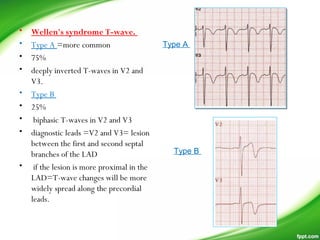
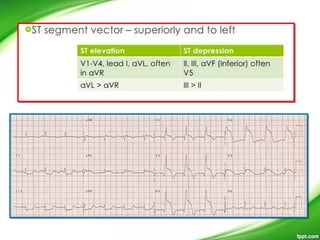
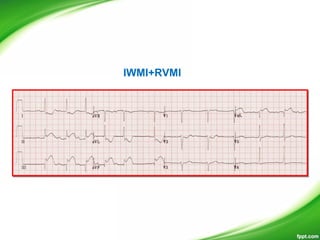
This document discusses various non-coronary causes of ST-elevation on electrocardiograms (ECGs) including ventricular aneurysms, pericarditis, early repolarization patterns, left ventricular hypertrophy, left bundle branch block, hypothermia, cardioversion, intraventricular hemorrhage, hyperkalemia, Brugada pattern, type 1C antiarrhythmic drugs, hypercalcemia, pulmonary embolism, hypothermia, myocarditis, and tumor invasion of the left ventricle. It then discusses left ventricular aneurysms, early repolarization, acute pericarditis, hyperkalemia, hypothermia, increased intracranial pressure, Brugada syndrome, Tak


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




