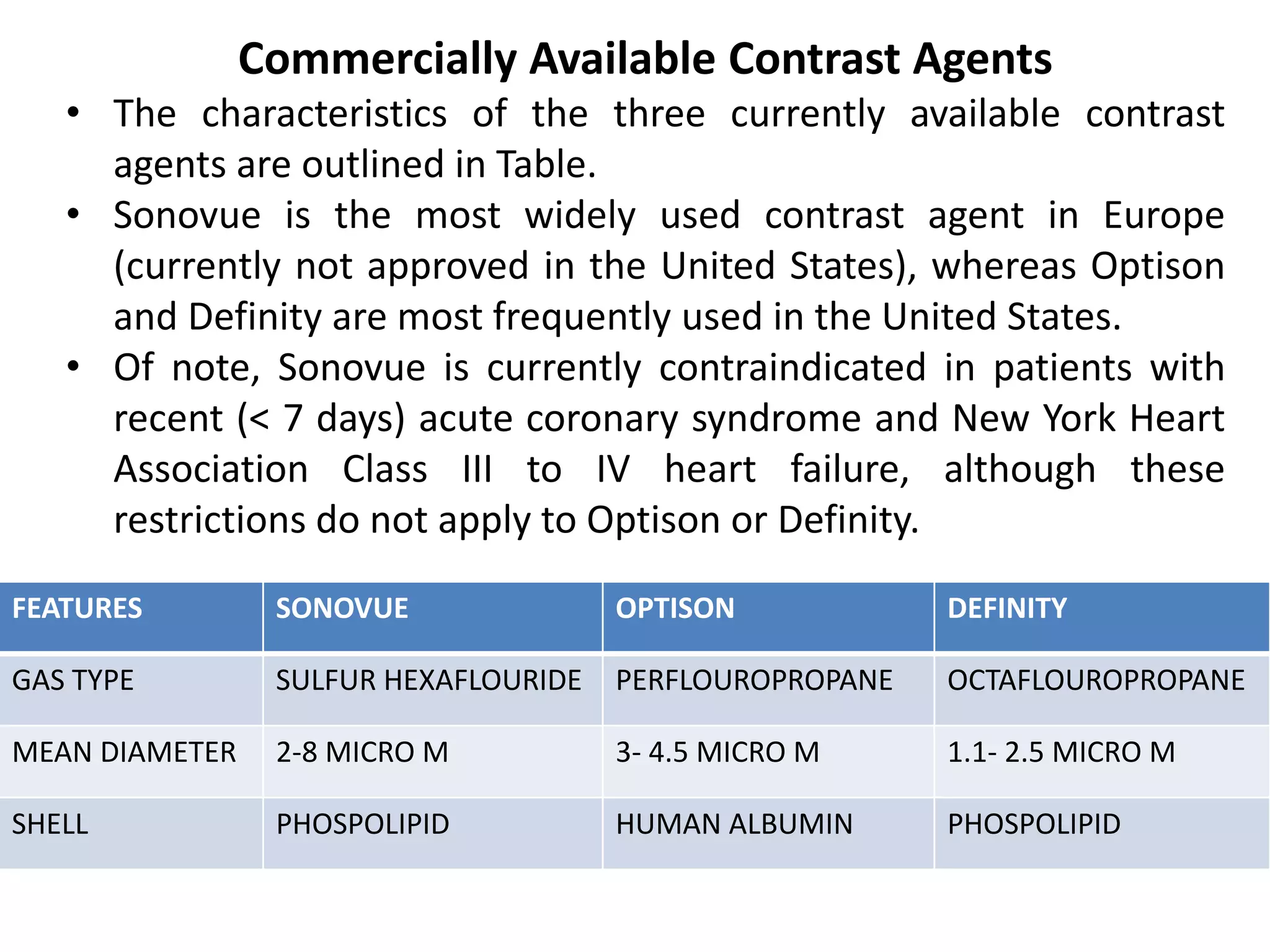
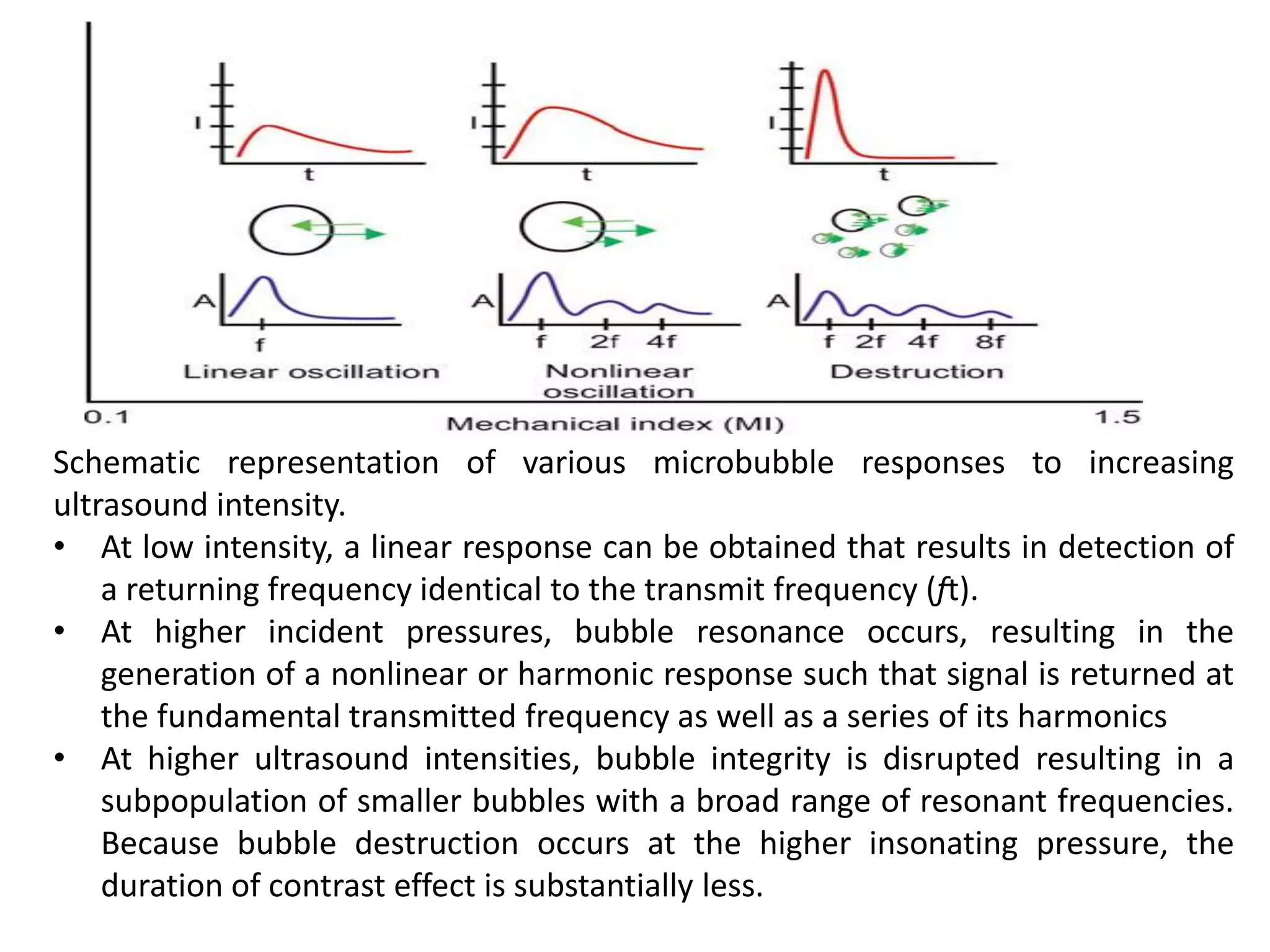
Contrast echocardiography uses microbubble ultrasound contrast agents to improve image quality. These microbubbles remain in the intravascular space and allow for assessment of cardiac structure, function, and perfusion. Second generation contrast agents use an inert gas encapsulated by albumin or phospholipid shells. They interact with ultrasound by reflecting at fundamental frequencies and resonating to produce harmonic frequencies. Continuous infusion provides steady contrast levels needed for perfusion assessment. Contrast echocardiography is a non-invasive technique that improves evaluation of the heart.