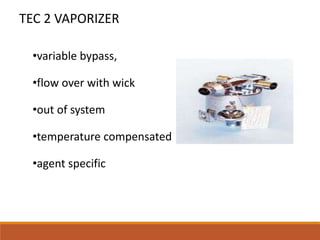
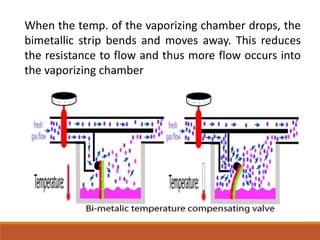
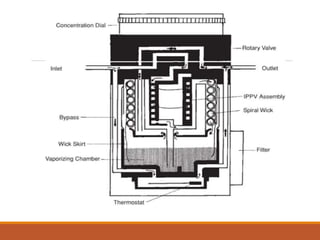
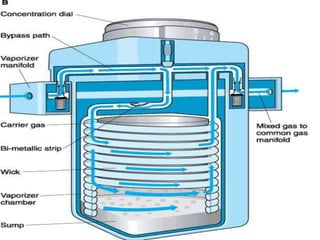
The document discusses different types of vaporizers used in anesthesia from Tec 1 to Tec 5. It describes the key parts, working, advantages and disadvantages of each vaporizer. Tec 1 was the earliest vaporizer introduced in 1956. Modern vaporizers like Tec 5 are variable bypass, temperature compensated, concentration calibrated and agent specific. They have improved safety features like internal baffles and locking mechanisms to prevent errors. The document also reviews the standards for vaporizers and procedures for filling and draining them.

































































![Vaporizer and Inhalational Anesthetics [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/vaporizerandinhalationalanestheticsautosaved-240829050532-cbdc4abd-thumbnail.jpg?width=640&height=640&fit=bounds)



























