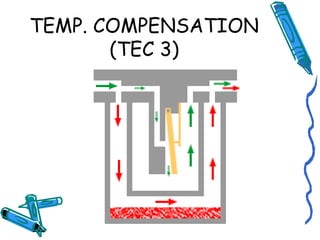
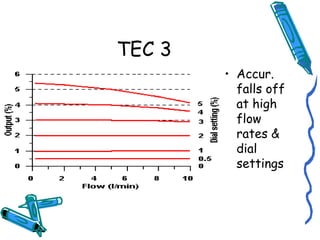
This document defines key concepts related to vaporisers such as vapor, vapor pressure, boiling point, and defines a vaporiser as an instrument that facilitates the change of a liquid anaesthetic into a vapor and adds a controlled amount to gas flow. It discusses factors that affect vaporiser performance such as carrier gas composition, temperature, back pressure and flow rate. It also classified vaporisers based on methods of regulating concentration and vaporization, and location in the breathing system. Modifications to vaporisers to address issues related to back pressure are described.
![EMO(ctd)
• Thermocompensation mechanism at outlet
of v.c.
– metal bellows with liquid Ether[ether capsule]
& connected to plunger
– temp. range; 15-29 degree Celsius
• Water jacket serves as heat reservoir
Checks
(1) check level indicator-put “in transit”-invert –
chould fall to full
(2) close outlet- connect OIB to inlet- put”in
transit”- press bellows- open filler –no air
should escape
(3) release filler-set at 10% -rpt above
(4) attach bellows to outlet-block inlet –set at 2
% -suck air – should hear a hissing if safety
release valve is working](https://image.slidesharecdn.com/vaporizersdr-140531012411-phpapp02/85/Vaporizers-dr-anju-bhalotra-66-320.jpg)





































































![Vaporizer and Inhalational Anesthetics [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/vaporizerandinhalationalanestheticsautosaved-240829050532-cbdc4abd-thumbnail.jpg?width=640&height=640&fit=bounds)














































