Downloaded 32 times
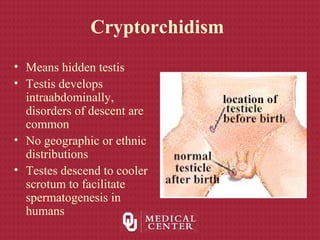


1) Cryptorchidism, or undescended testes, occurs when the testes fail to descend into the scrotum. This can be due to abnormalities in testicular descent during embryonic development between 5-9 months of gestation. 2) The incidence of cryptorchidism is about 3-5% in full term infants but higher in premature infants. By age 1, about 1-1.5% of boys will have undescended testes. 3) Cryptorchidism increases the risk of testicular cancer. About 10% of all testicular cancers occur in undescended testes. The risk is higher for intra-abdominal versus inguinal undesc























































































