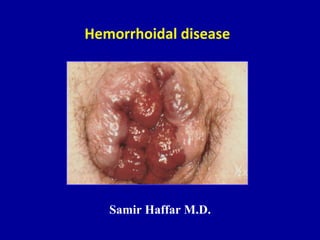
This document discusses hemorrhoidal disease, including definitions, incidence, pathogenesis, classification, symptoms, and treatment options. It defines hemorrhoids as dilated vascular channels located in three constant locations in the anus. Hemorrhoidal disease is manifested by prolapse, bleeding, and itching. Treatment options discussed include sclerosing injections, infrared photocoagulation, rubber band ligation, and hemorrhoidectomy. The preferences for treatment are outlined based on the degree of hemorrhoids.