Downloaded 14 times
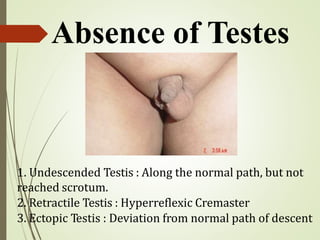

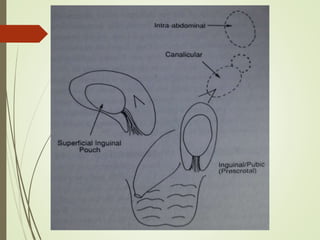


The document discusses the condition of undescended testes (cryptorchidism), outlining types such as undescended, retractile, and ectopic testes, along with their embryological development and factors influencing their descent. It highlights clinical features, management strategies including surgery options like orchidopexy, and considerations for palpable versus impalpable testes. The document also mentions potential complications and the need for careful evaluation based on the age and condition of the child.