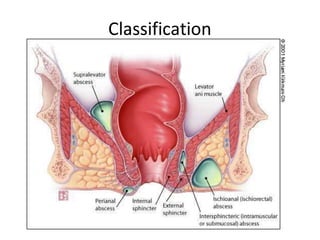
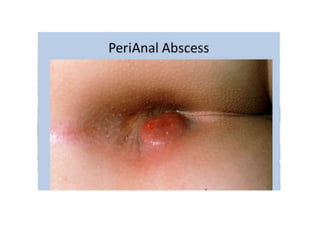
Anorectal abscesses, primarily caused by E. coli infections from anal gland issues, are common in diabetics and immunocompromised individuals. They can be classified into perianal (60%), ischiorectal (30%), and others, with treatments including incision and drainage, antibiotics, and analgesics. Complications may include fistula formation and recurrences, with approximately 50% of patients potentially developing an anal fistula after drainage.