




























![Remodeling
A. Normal B. Flattening C. Erosion D. Osteophytes E. Bone remodel
mand. fossa
ALVES, N et al. Morphological Characteristics of the Temporomandibular Joint Articular Surfaces in Patients with
Temporomandibular Disorders. Int. J. Morphol. [online]. 2013, vol.31, n.4 [citado 2016-11-13], pp.1317-1321.](https://image.slidesharecdn.com/tmjfindingsincbctmri-161205185144/75/Tmj-findings-in-cbct-amp-mri-39-2048.jpg)






![Remodeling: Subchondral cyst
ALVES, N et al. Morphological Characteristics of the Temporomandibular Joint Articular Surfaces in Patients with
Temporomandibular Disorders. Int. J. Morphol. [online]. 2013, vol.31, n.4 [citado 2016-11-13], pp.1317-1321.](https://image.slidesharecdn.com/tmjfindingsincbctmri-161205185144/75/Tmj-findings-in-cbct-amp-mri-47-2048.jpg)
![Remodeling: Osteophyte with ‘joint mice’
ALVES, N et al. Morphological Characteristics of the Temporomandibular Joint Articular Surfaces in Patients with
Temporomandibular Disorders. Int. J. Morphol. [online]. 2013, vol.31, n.4 [citado 2016-11-13], pp.1317-1321.](https://image.slidesharecdn.com/tmjfindingsincbctmri-161205185144/75/Tmj-findings-in-cbct-amp-mri-48-2048.jpg)



















































![References:
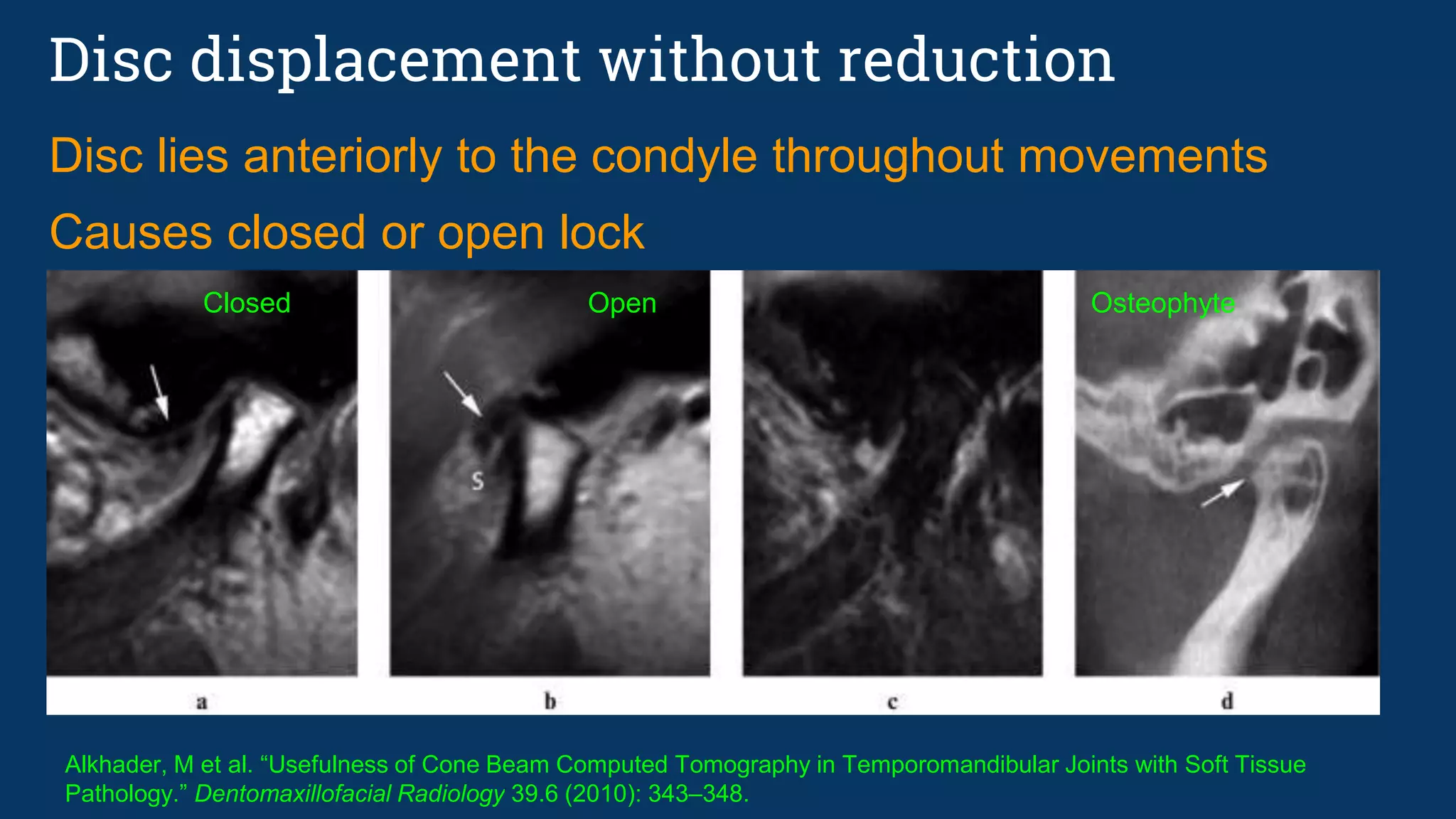
16. Alkhader, M et al. “Usefulness of Cone Beam Computed Tomography in Temporomandibular Joints with Soft Tissue
Pathology.” Dentomaxillofacial Radiology 39.6 (2010): 343–348.
17. Lee DY, Kim YJ, Song YH, Lee NH, Lim YK, Kang ST, Ahn SJ.; Comparison of bony changes between panoramic
radiograph and cone beam computed tomographic images in patients with temporomandibular joint disorders;
Korean J Orthod. 2010 Dec;40(6):364-372. Published online 2010 December
18. ALVES, N et al. Morphological Characteristics of the Temporomandibular Joint Articular Surfaces in Patients with
Temporomandibular Disorders. Int. J. Morphol. [online]. 2013, vol.31, n.4 [citado 2016-11-13], pp.1317-1321.
19. Sodhi A, Naik S, Pai A, Anuradha A. Rheumatoid arthritis affecting temporomandibular joint. Contemporary Clinical Dentistry.
2015;6(1):124-127. doi:10.4103/0976-237X.149308.
20. Al-Khalisy HM, Nikiforov I, Mansoora Q, Goldman J, Cheriyath P. Septic Arthritis in the Temporomandibular Joint. North
American Journal of Medical Sciences. 2015;7(10):480-482. doi:10.4103/1947-2714.168678.
21. http://roentgenrayreader.blogspot.com/2011/07/synovial-chondromatosis-of.html
22. Lim SW, Jeon SJ, Choi SS, Choi KH. Synovial chondromatosis in the temporomandibular joint: a case with typical imaging
features and pathological findings. The British Journal of Radiology. 2011;84(1007):e215-e218. doi:10.1259/bjr/69067316.
23. Hegde RJ, Devrukhkar VN, Khare SS, Saraf TA. Temporomandibular joint ankylosis in child: A case report. J Indian Soc
Pedod Prev Dent 2015;33:166-9
24. Rheumatology Network
25. Marius Bredella, et al, Tenosynovial, Diffuse Type Giant Cell Tumor of the Temporomandibular Joint, Diagnosis and
Management of a Rare Tumor, Journal of Clinical Medicine Research, Vol. 7, No. 4, Apr 2015
26. Slide share: Nour-Eldin A., Nour-Eldin Mohammed
27. Dorrit W. Nitzan, The process of lubrication impairment and its involvement in temporomandibular joint disc displacement:
A theoretical concept, Journal of Oral and Maxillofacial Surgery, Volume 59, Issue 1, Pages 36-45
28. Yount, K, Osteoarthritis of TMJ, Practical Pain Management Dec, 2011](https://image.slidesharecdn.com/tmjfindingsincbctmri-161205185144/75/Tmj-findings-in-cbct-amp-mri-100-2048.jpg)


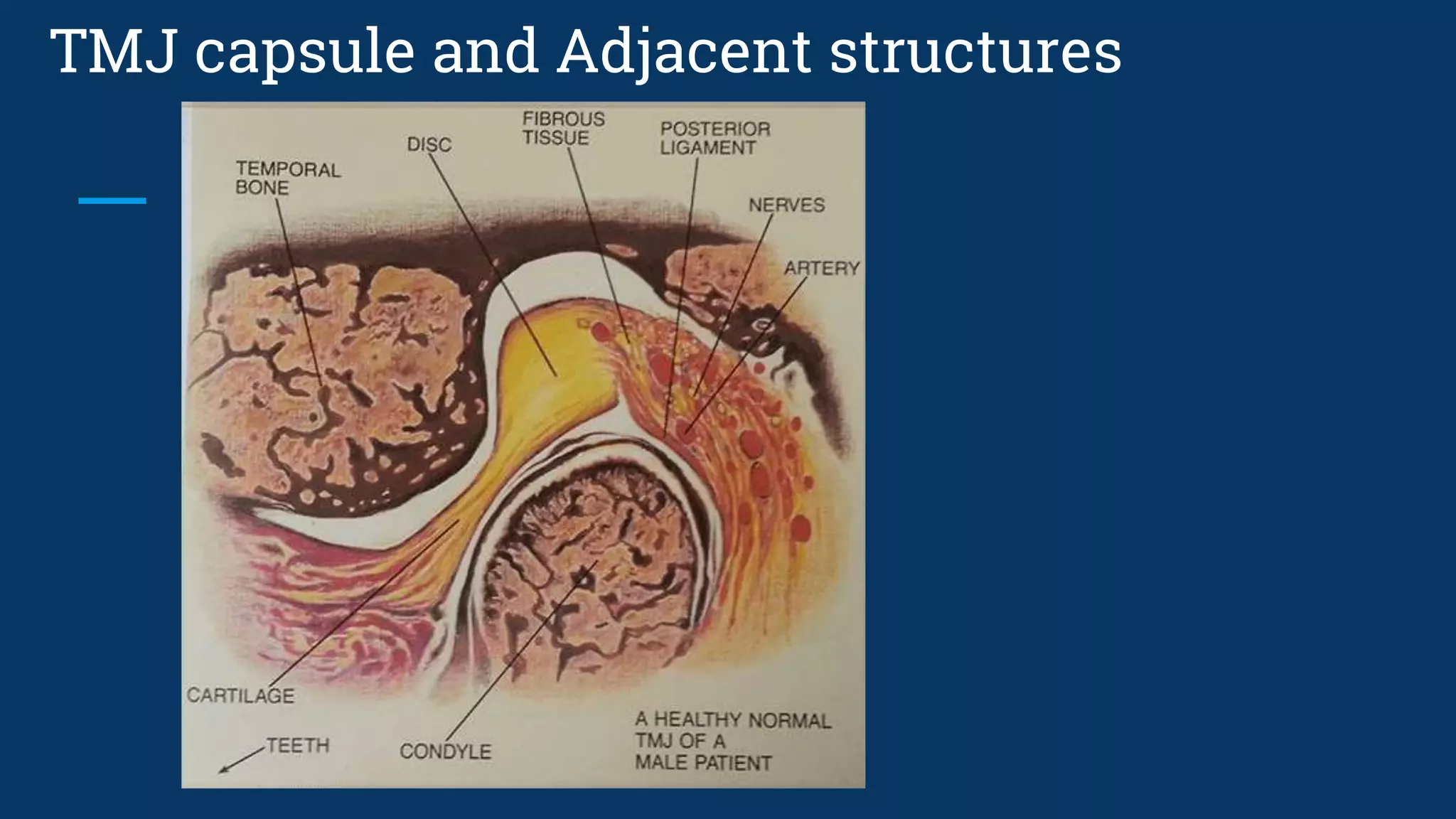
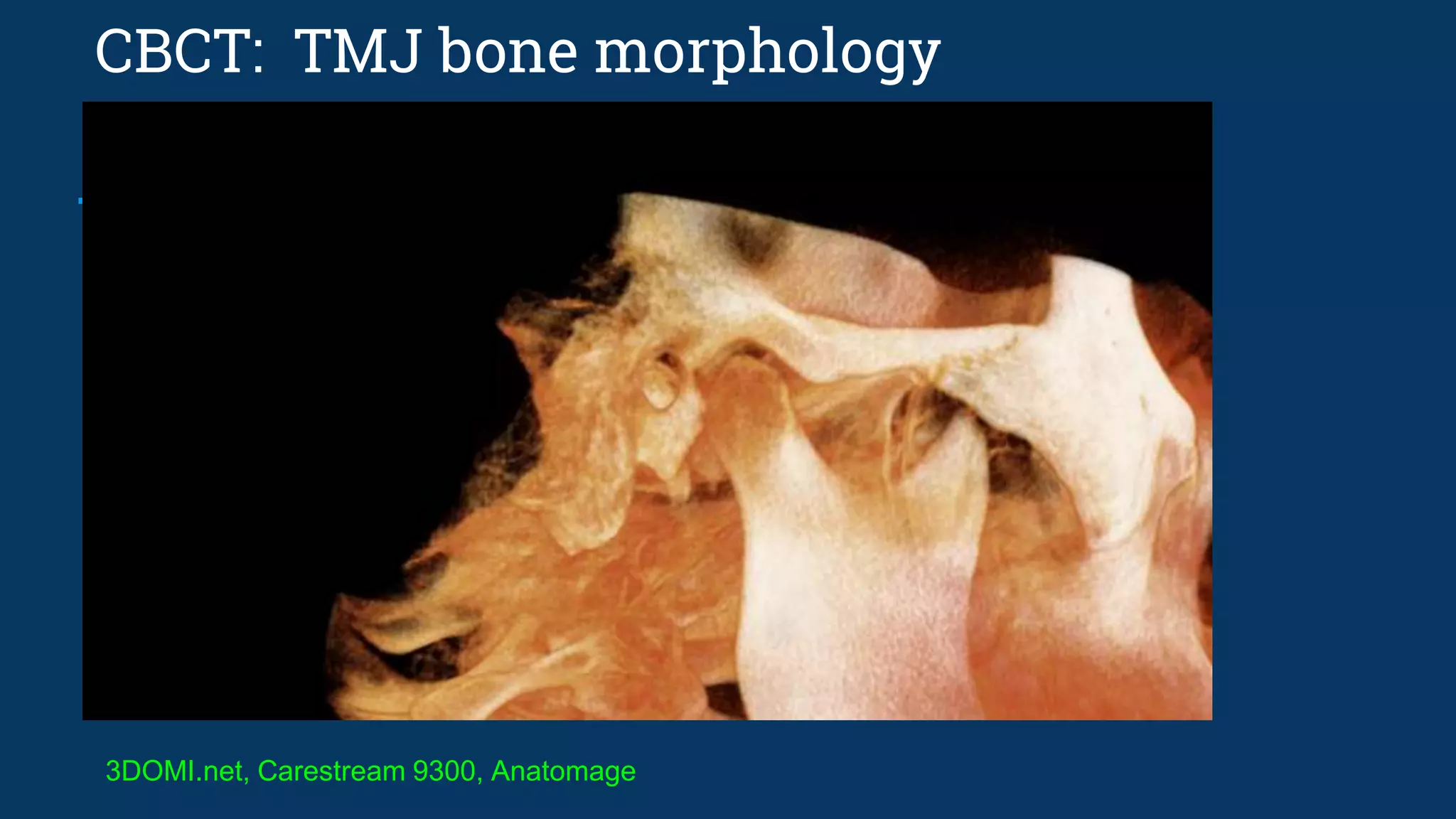
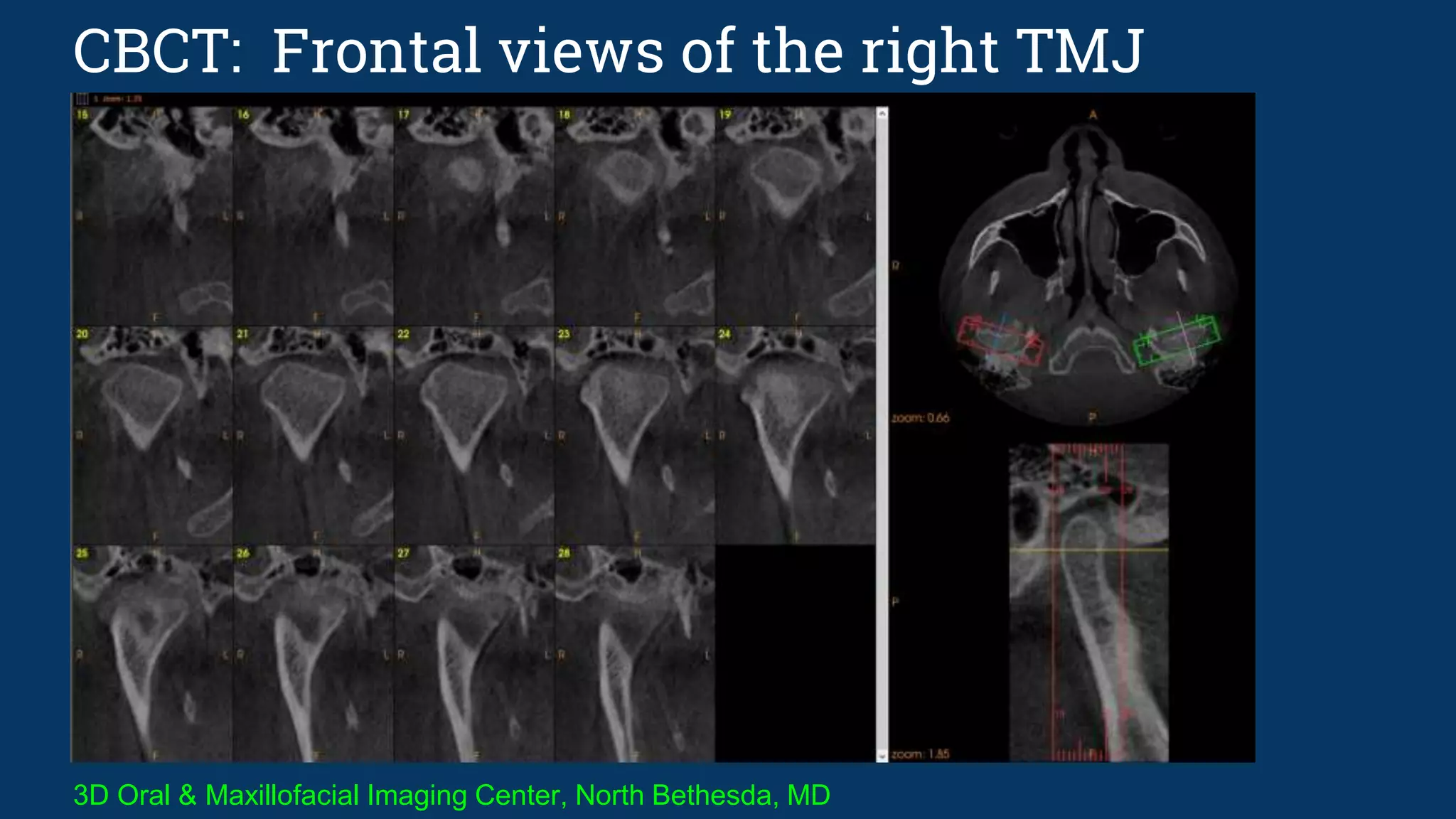
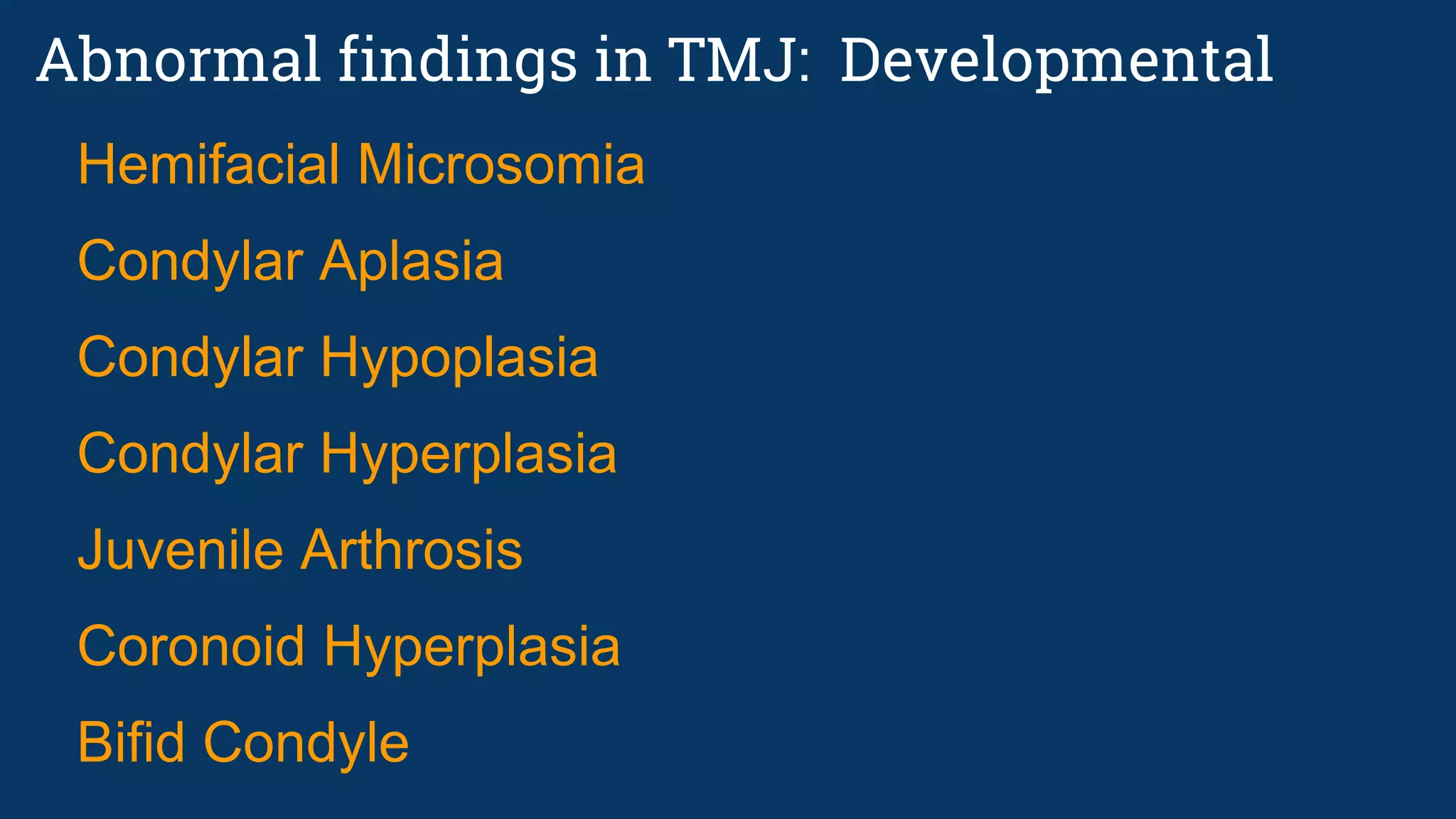
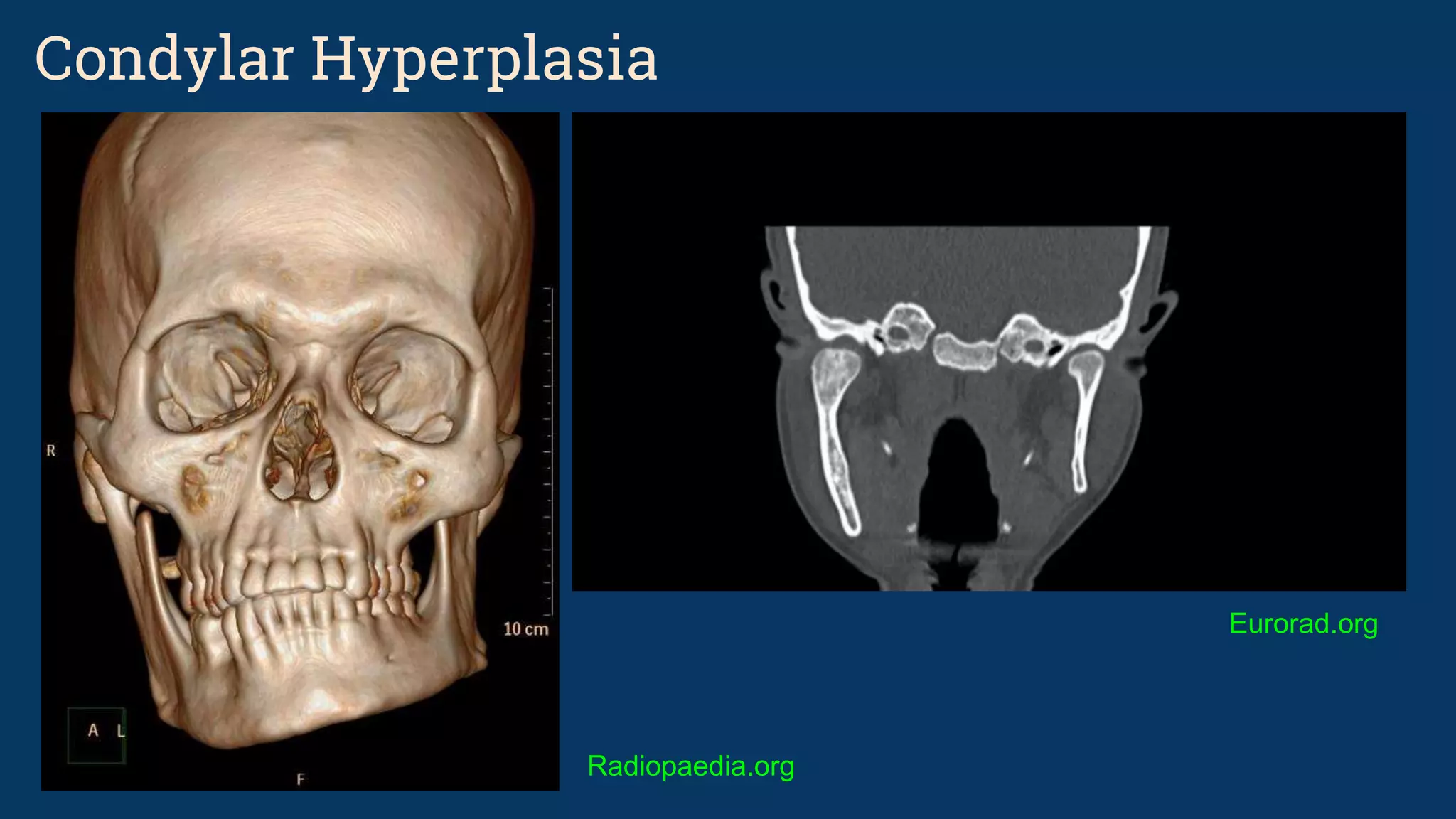
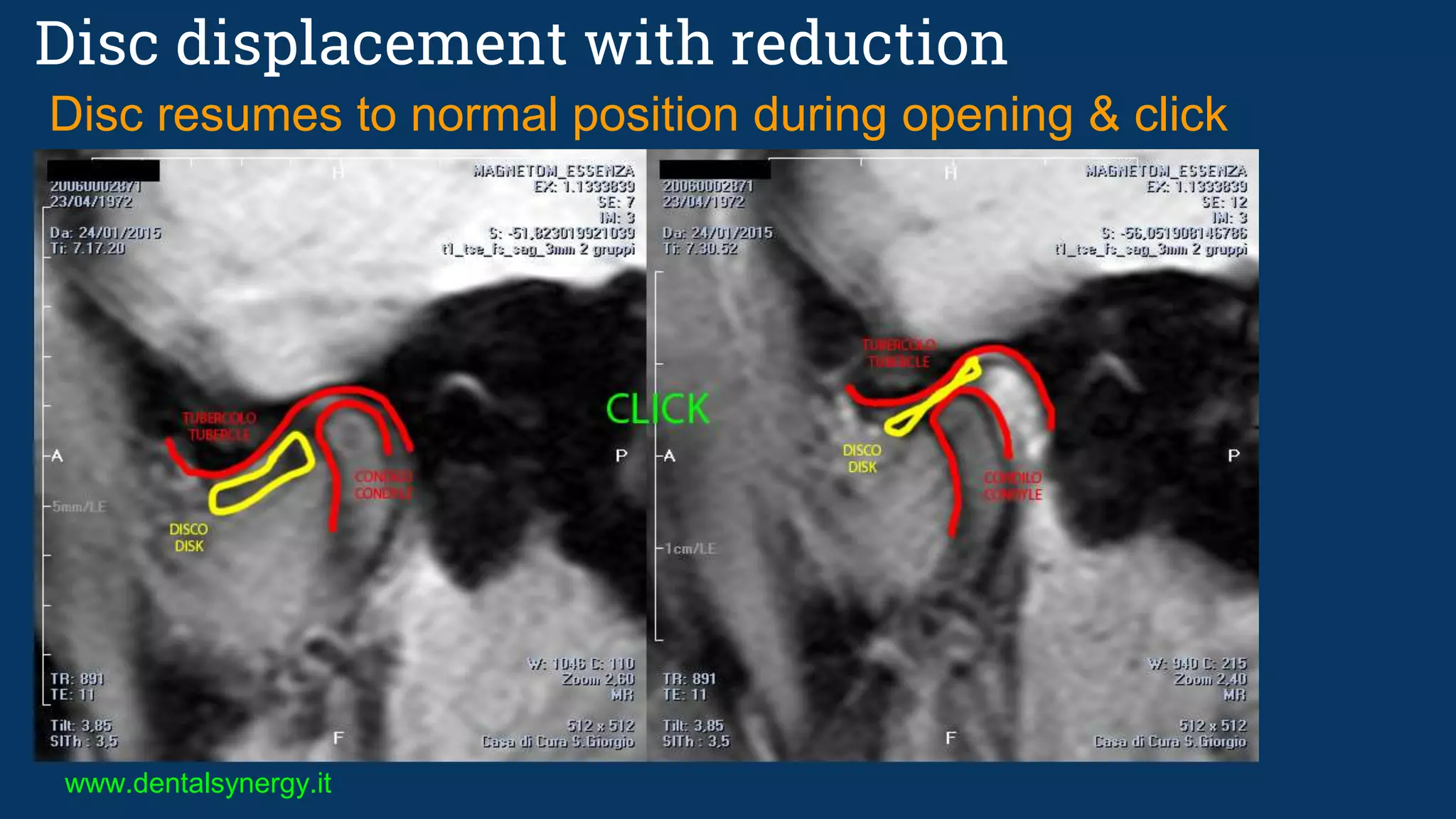
The document discusses various temporomandibular joint (TMJ) findings that can be seen on cone beam computed tomography (CBCT) and magnetic resonance imaging (MRI). It begins by describing the normal TMJ anatomy and capsule structures visible on imaging. It then discusses various abnormal and pathological TMJ findings that can be developmental, soft tissue related, or due to remodeling/arthritis. Developmental conditions covered include hemifacial microsomia, condylar aplasia, hypoplasia, and hyperplasia. Soft tissue abnormalities include internal derangements and disc displacements. Remodeling and arthritic changes described are flattening, erosion, osteophytes, sclerosis, and subchond






















































































