


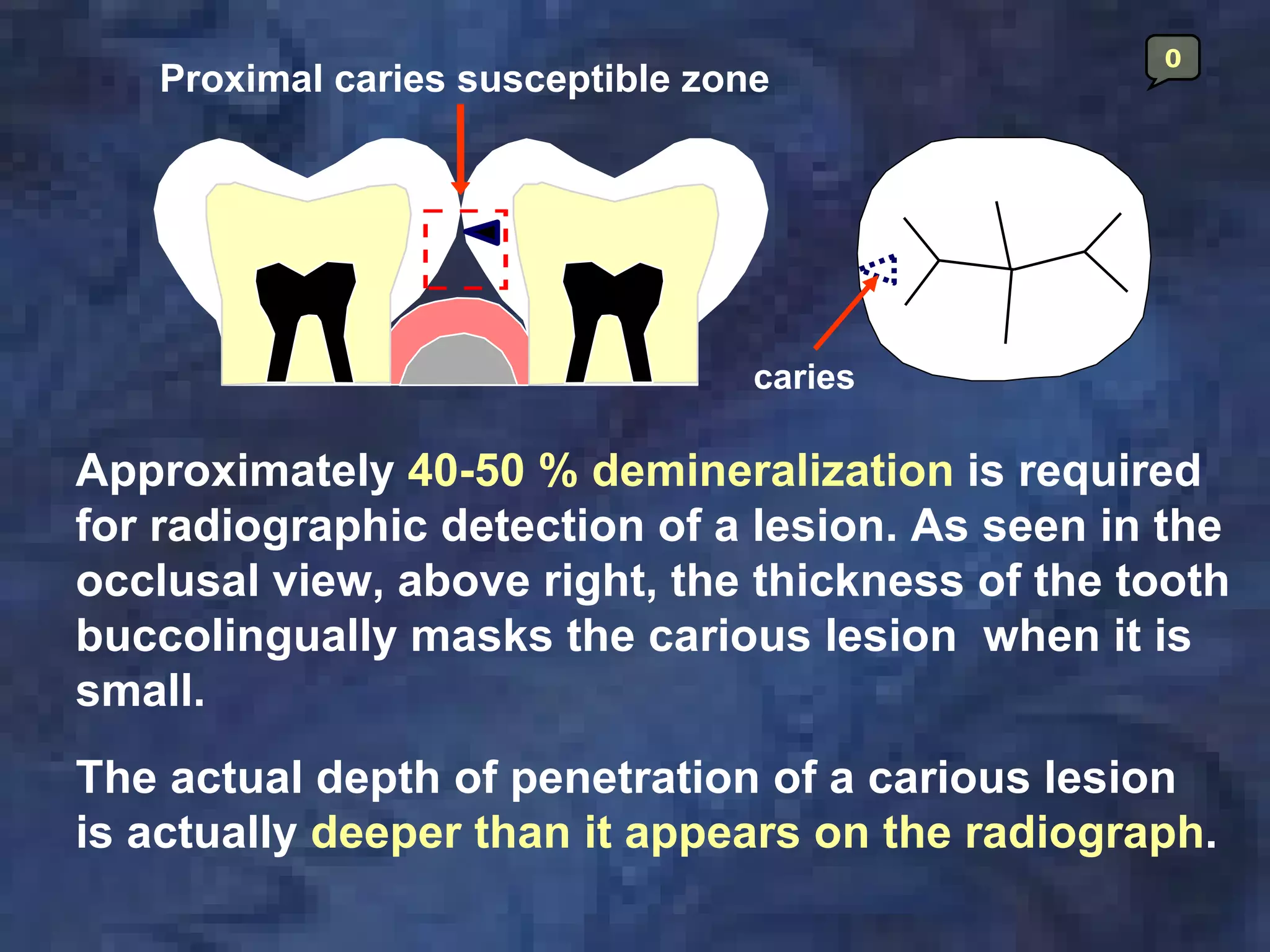
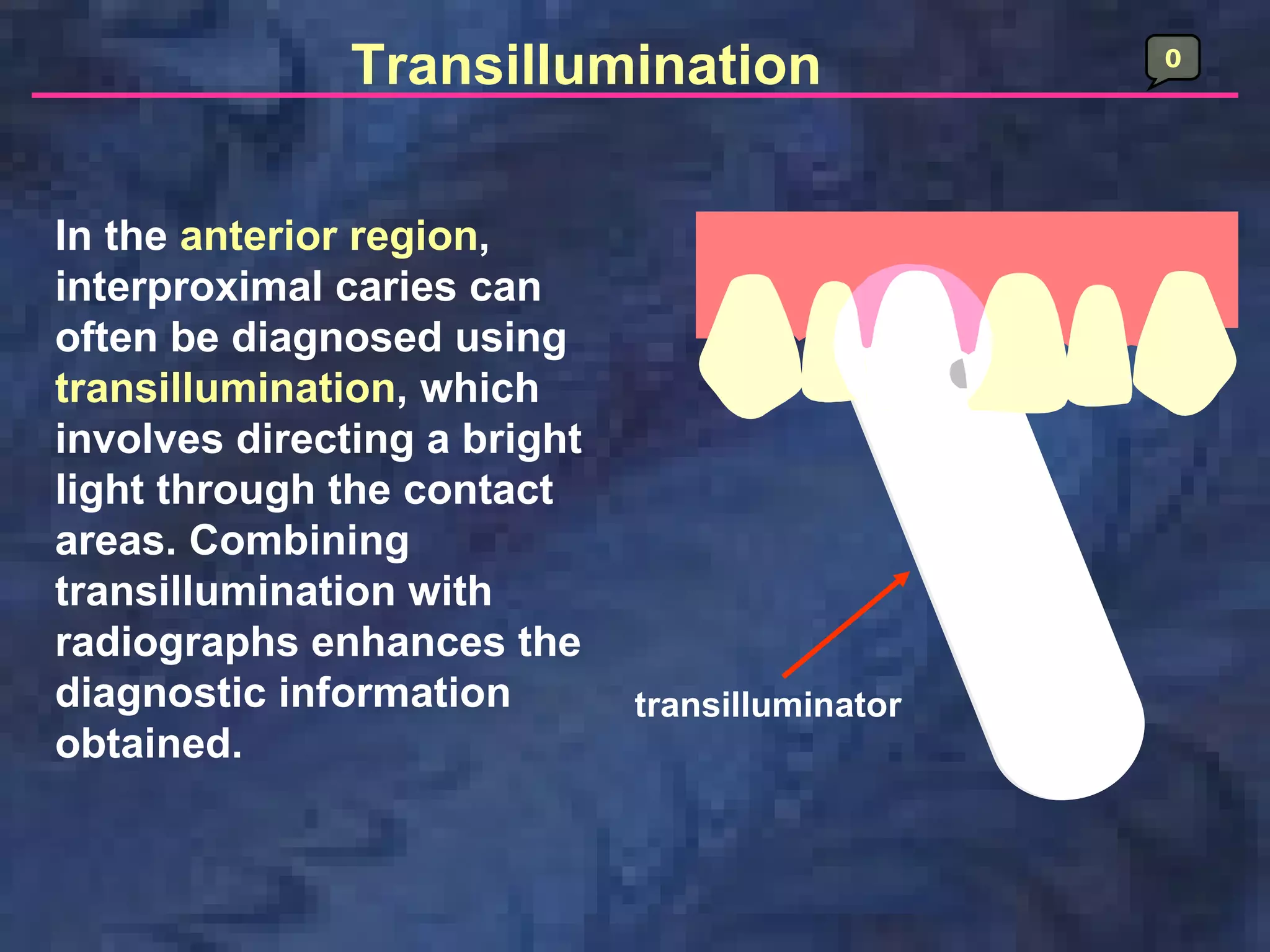
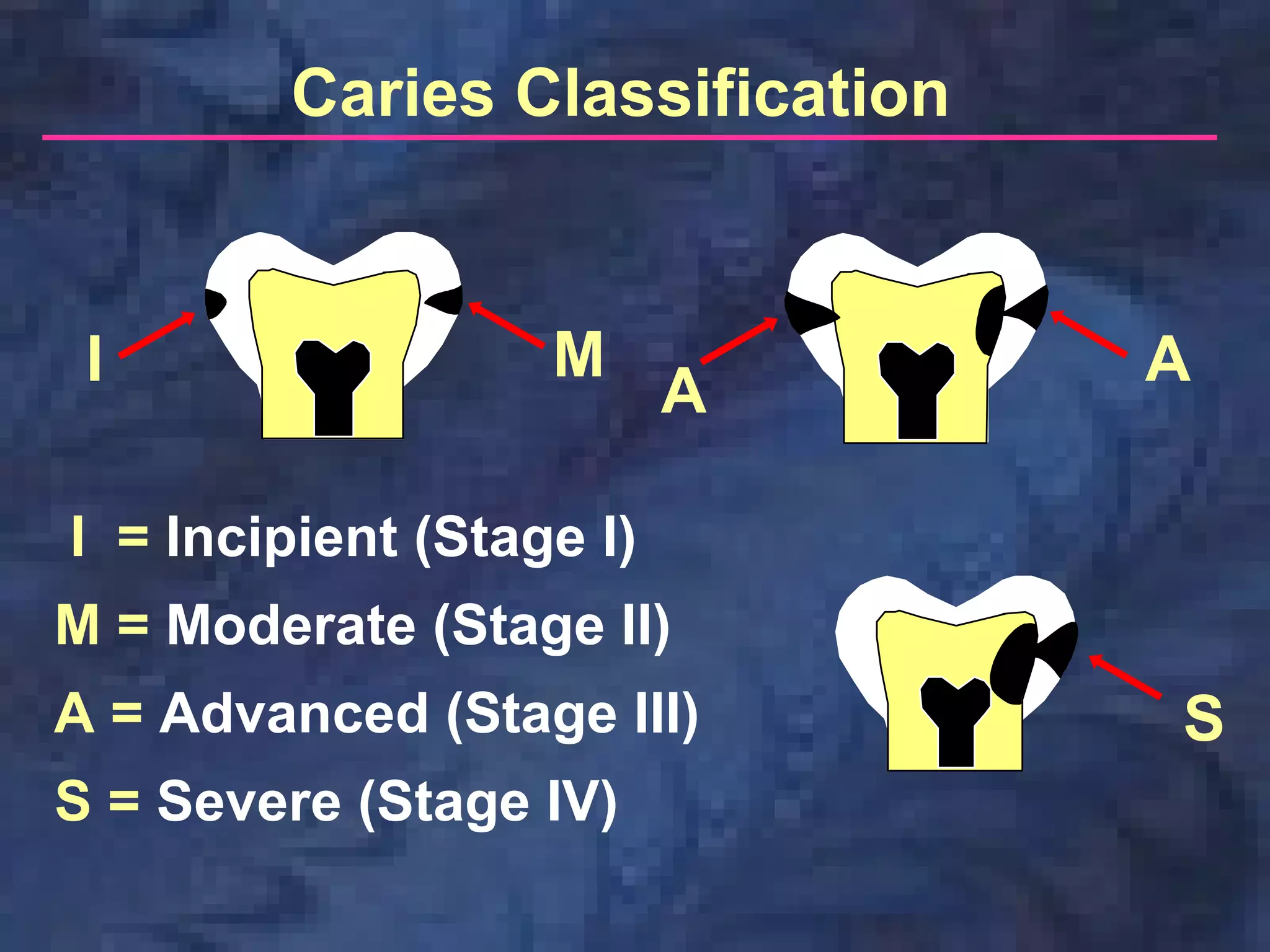




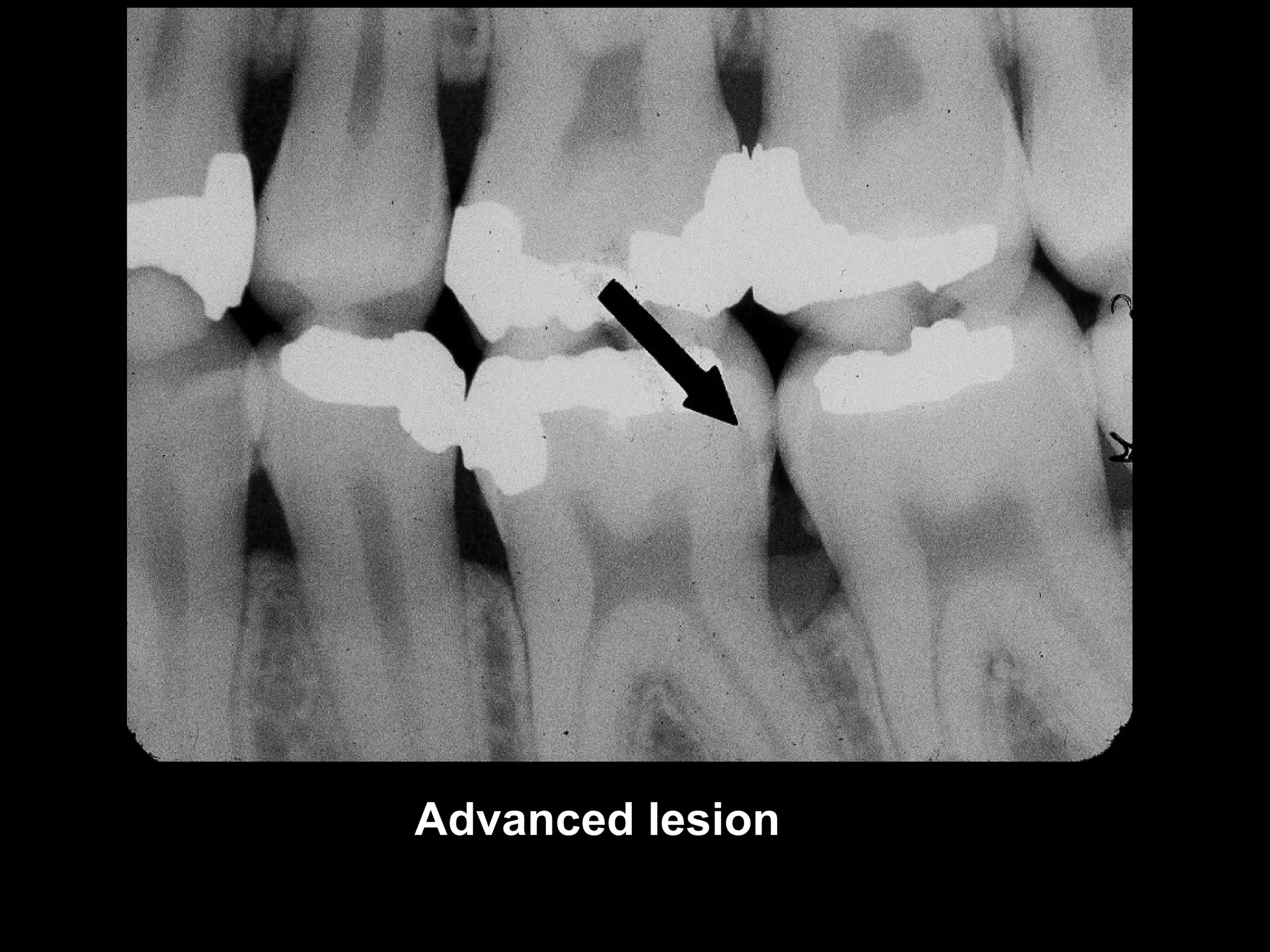
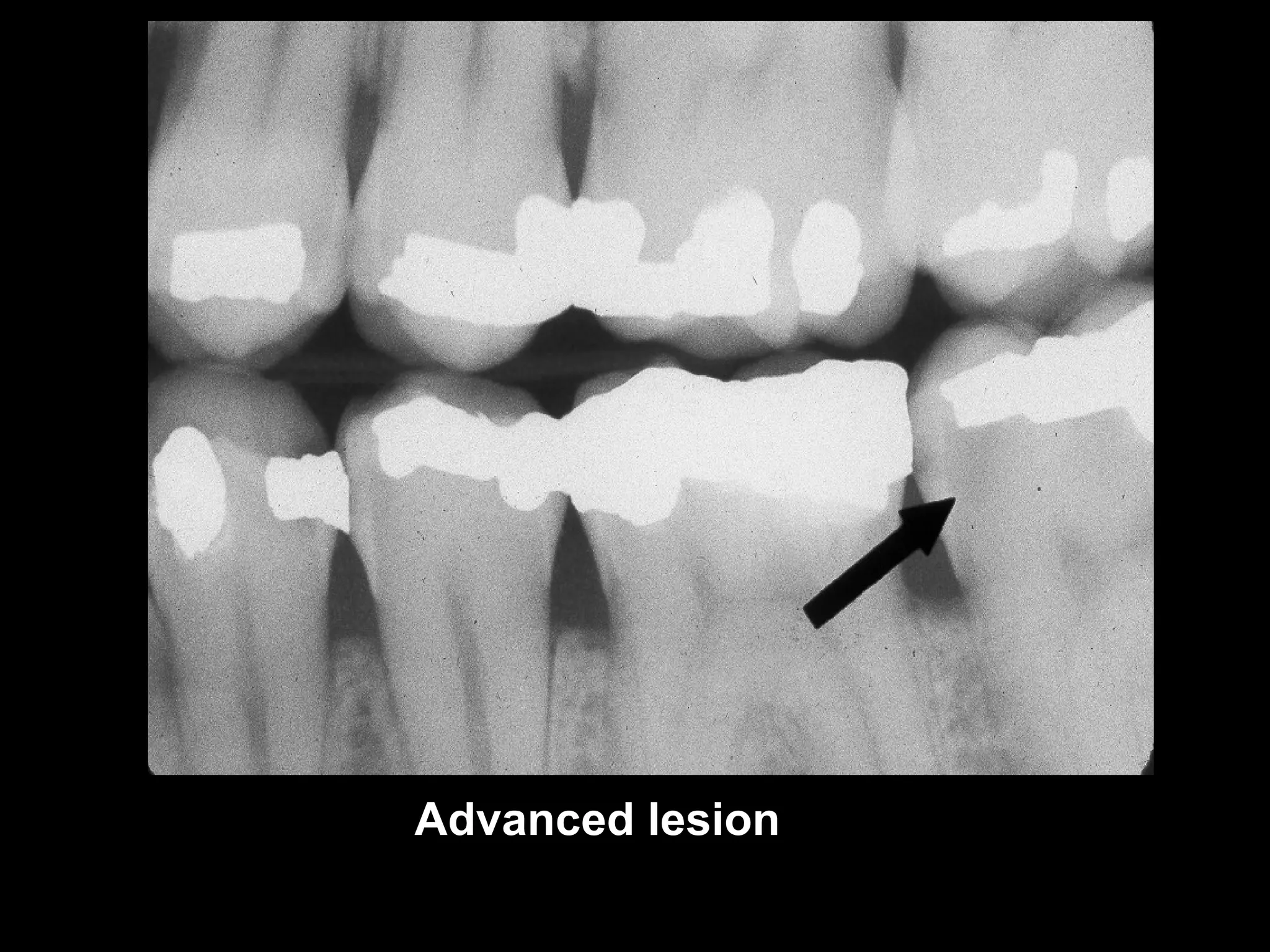
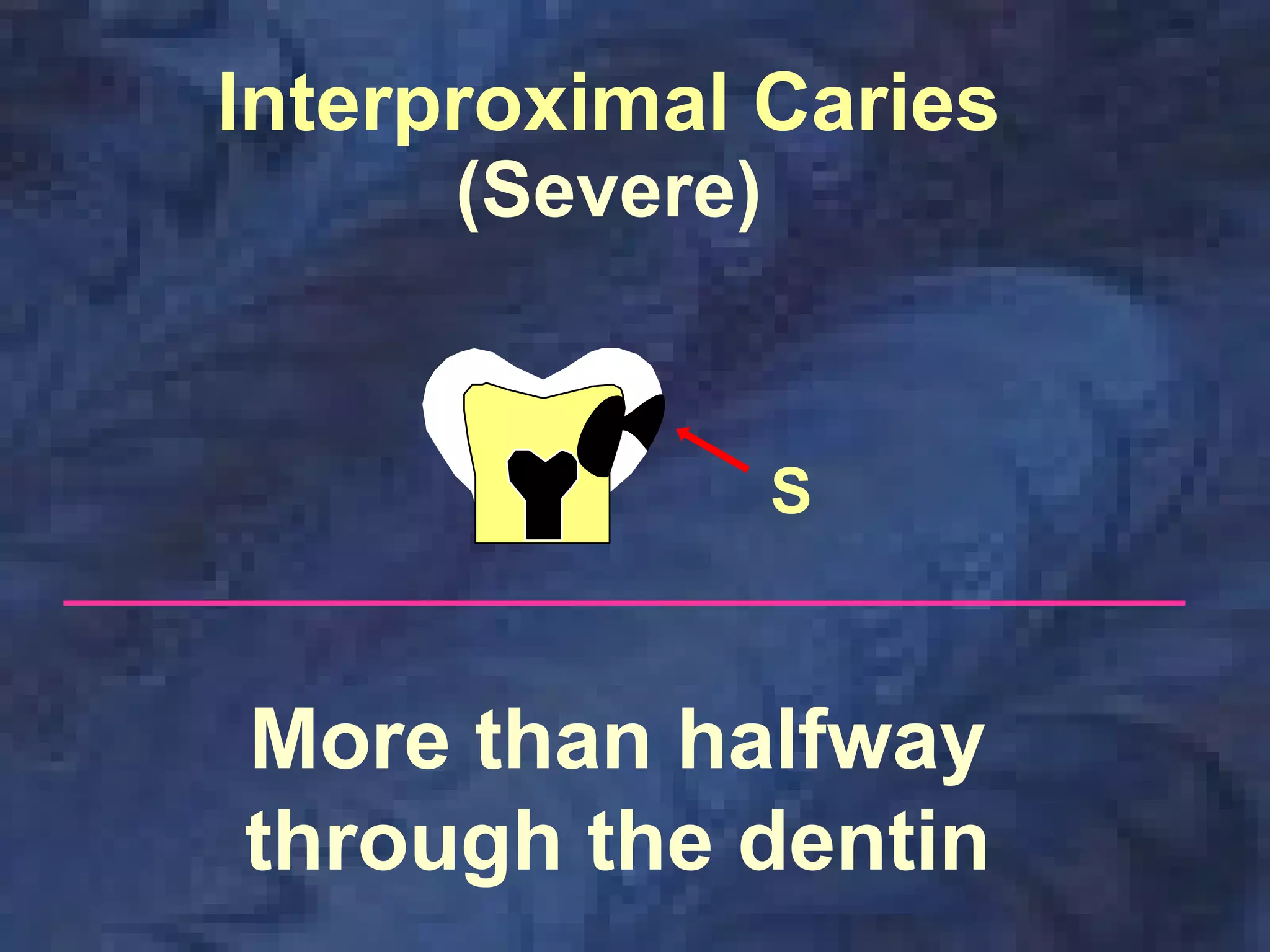

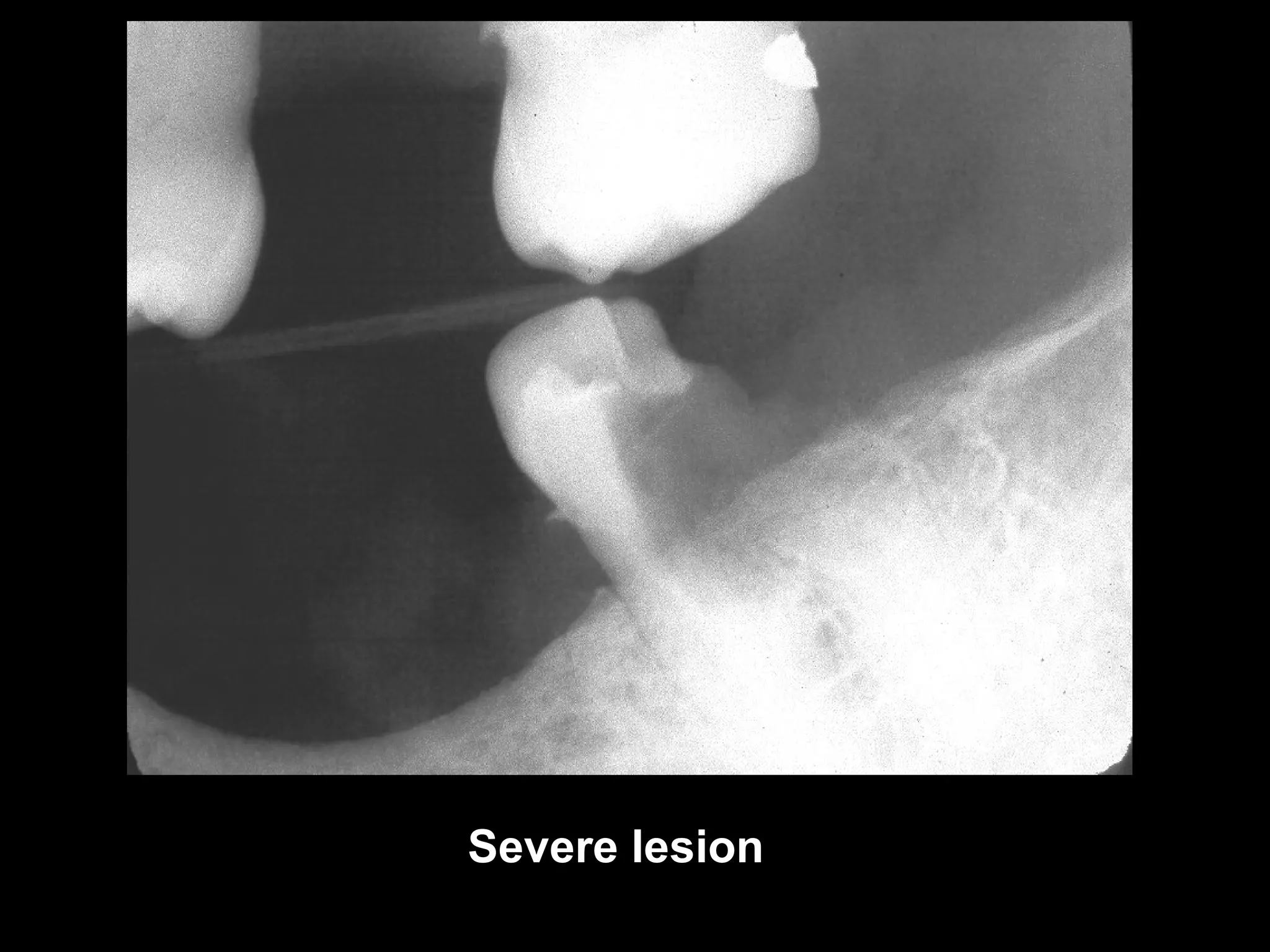



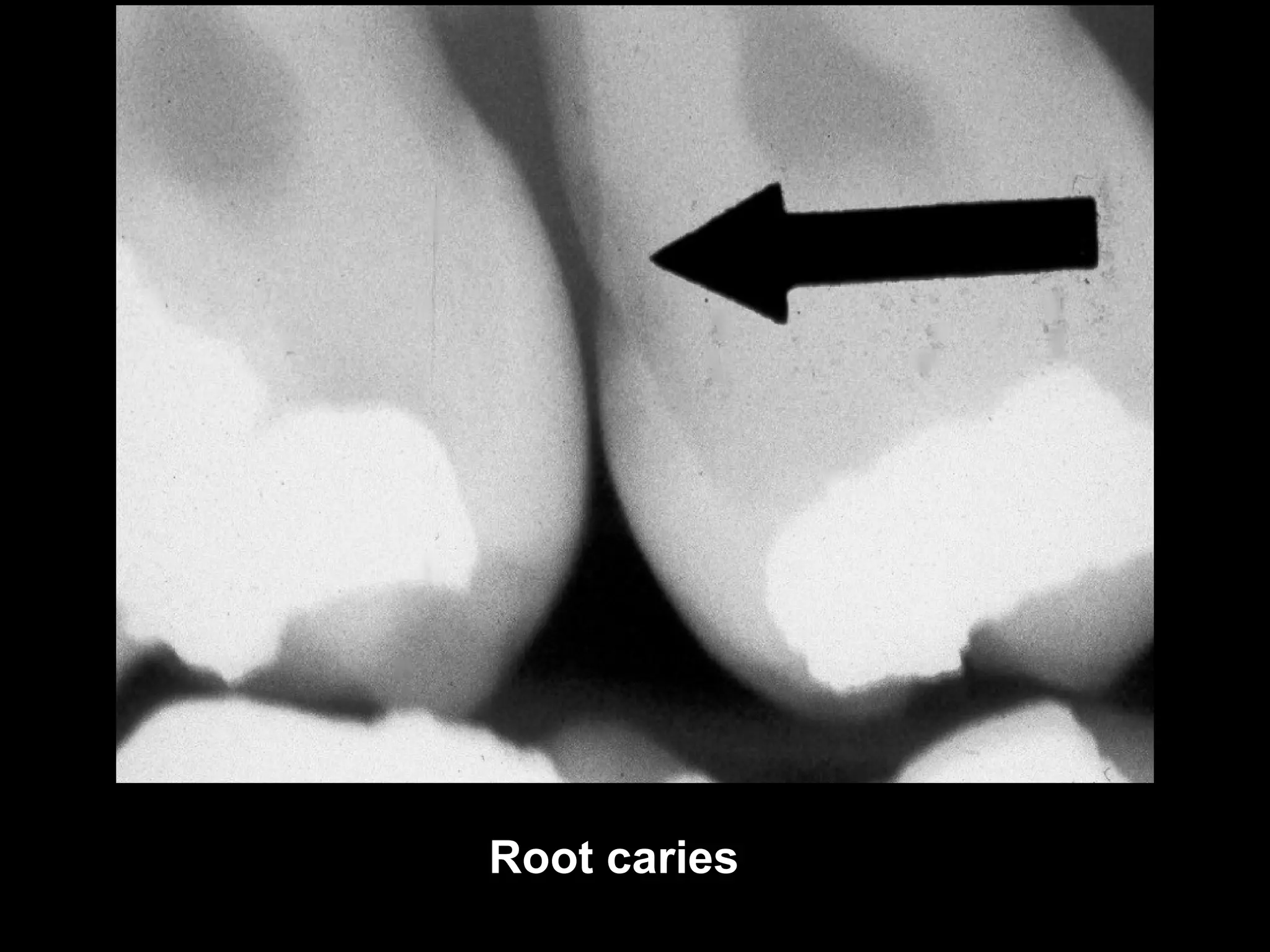


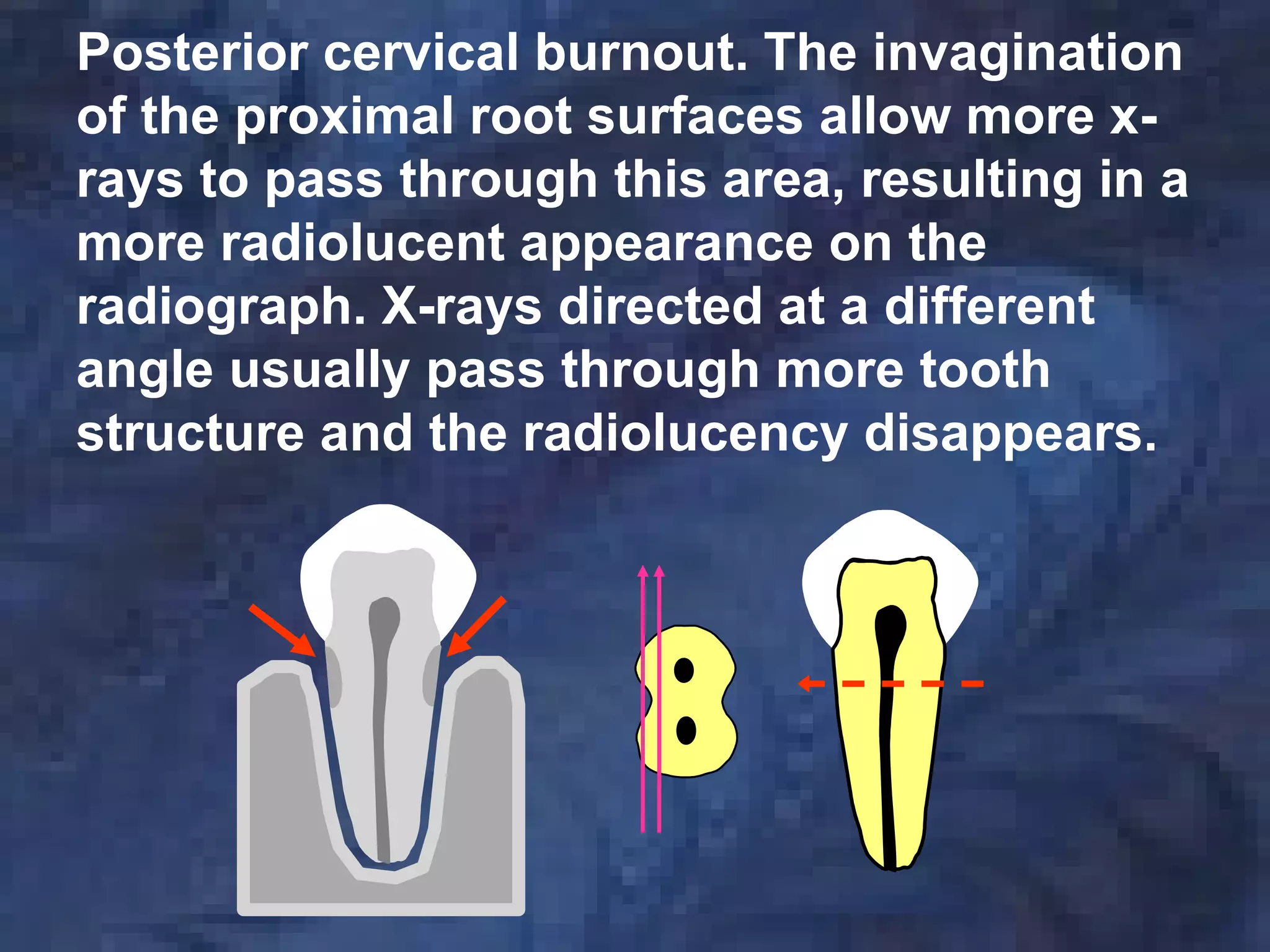
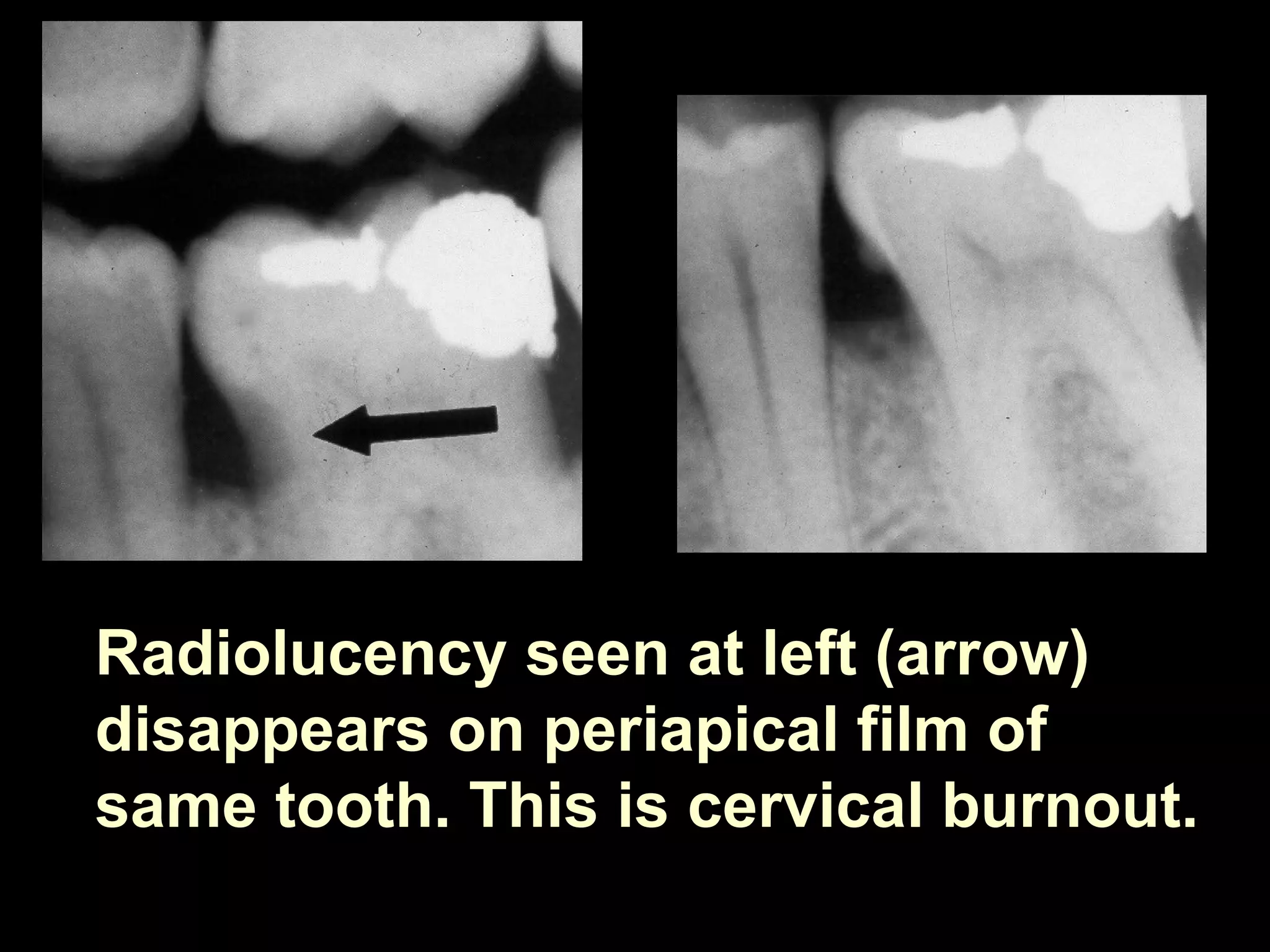



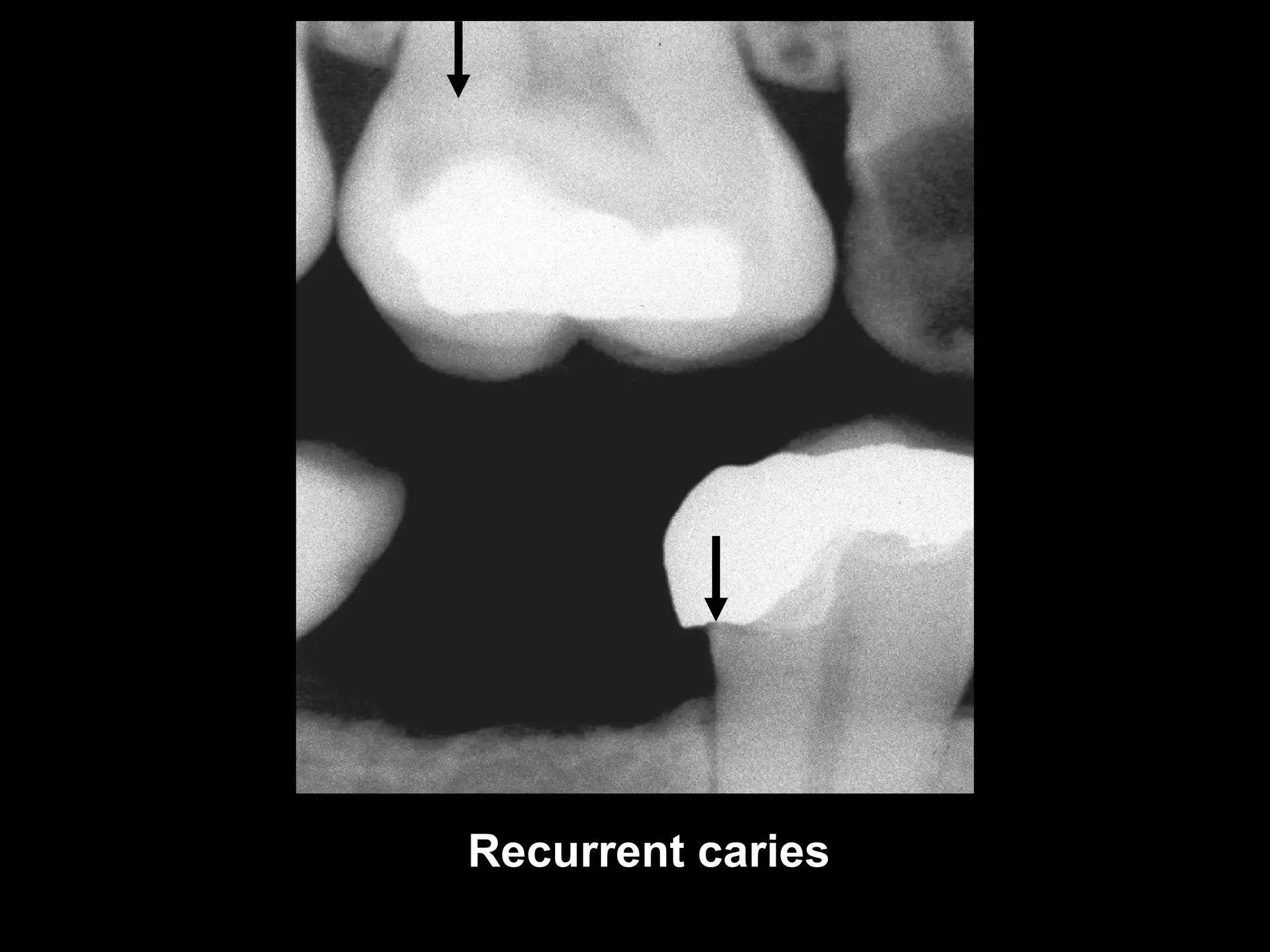
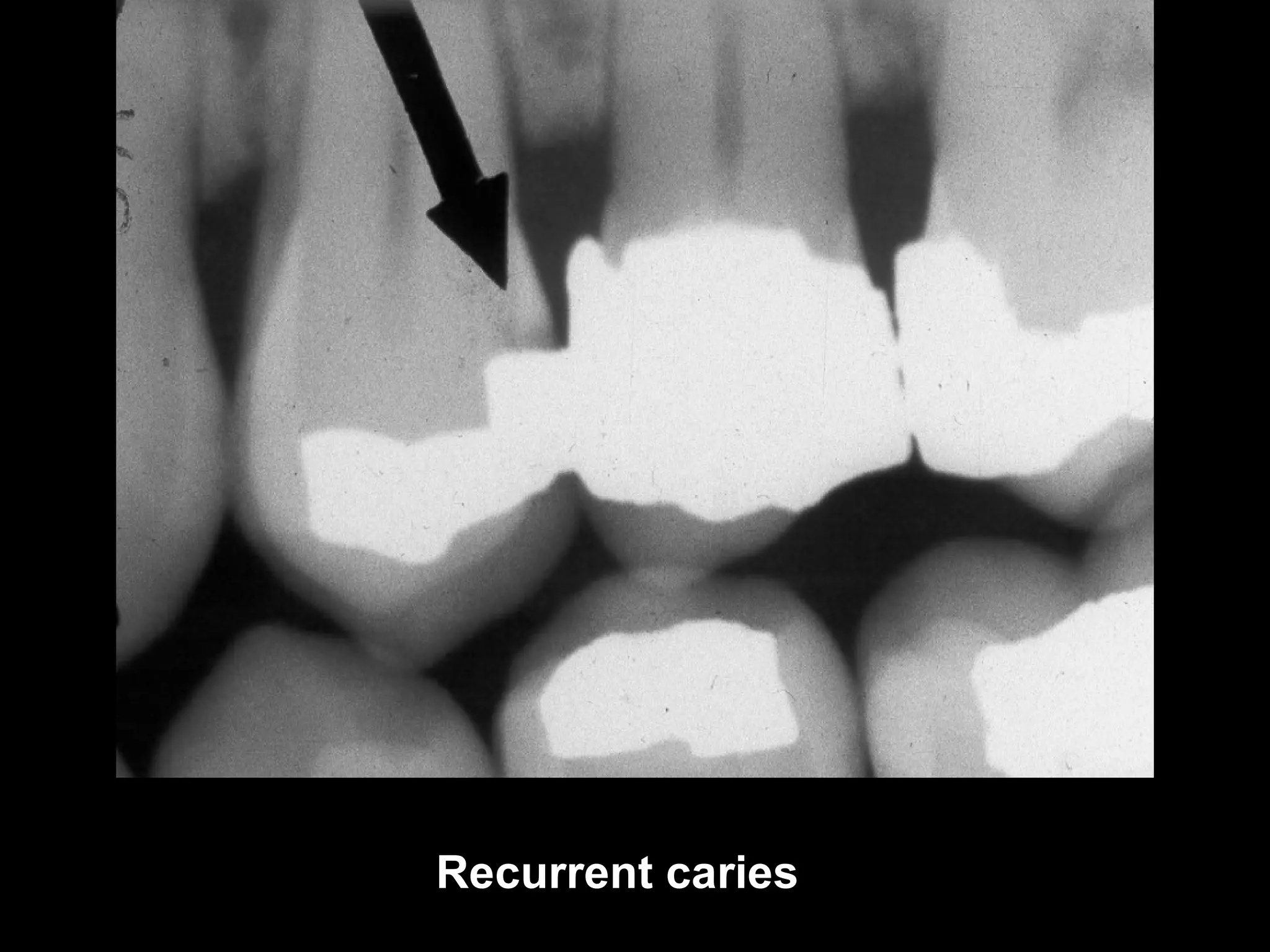
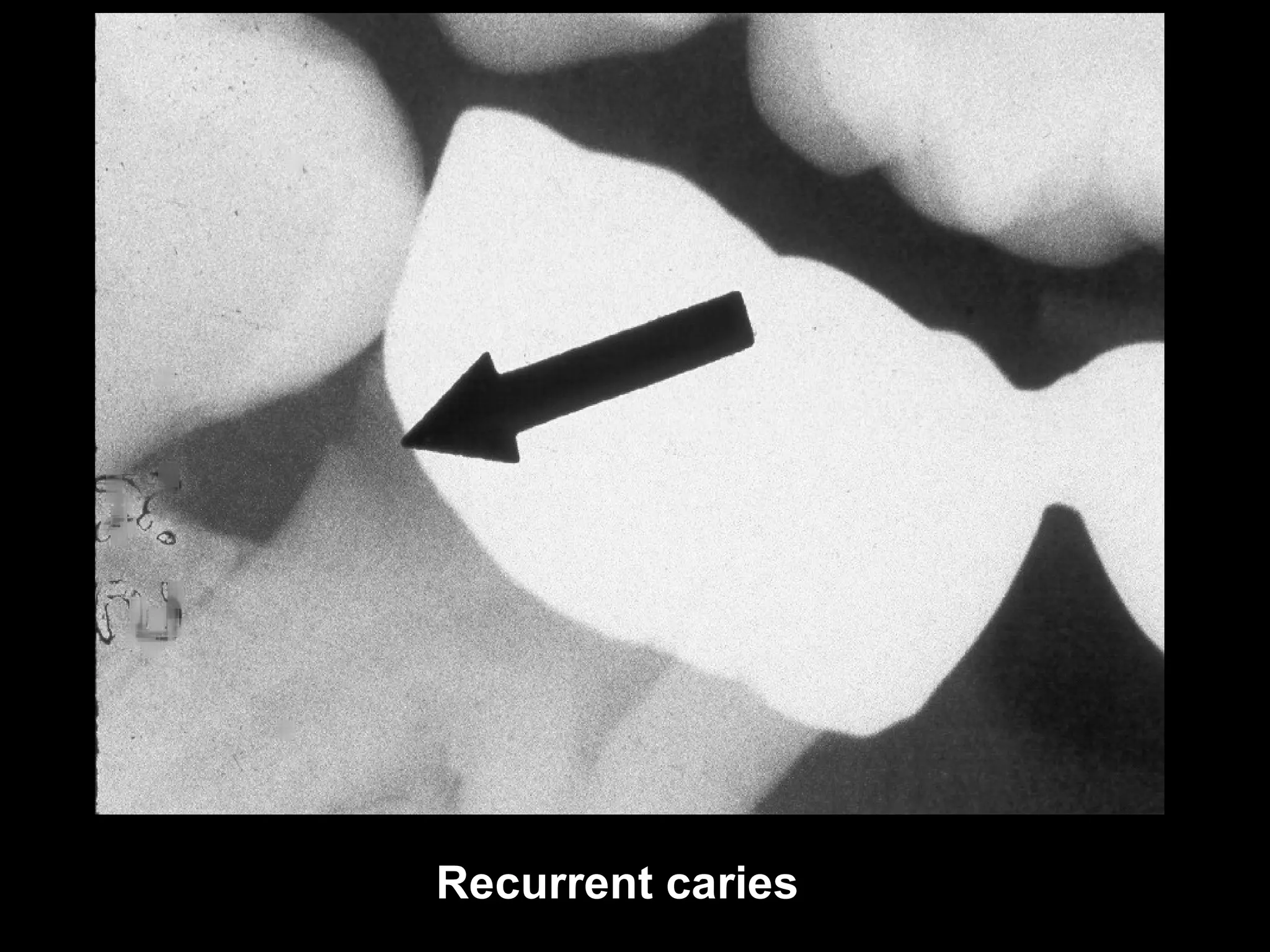

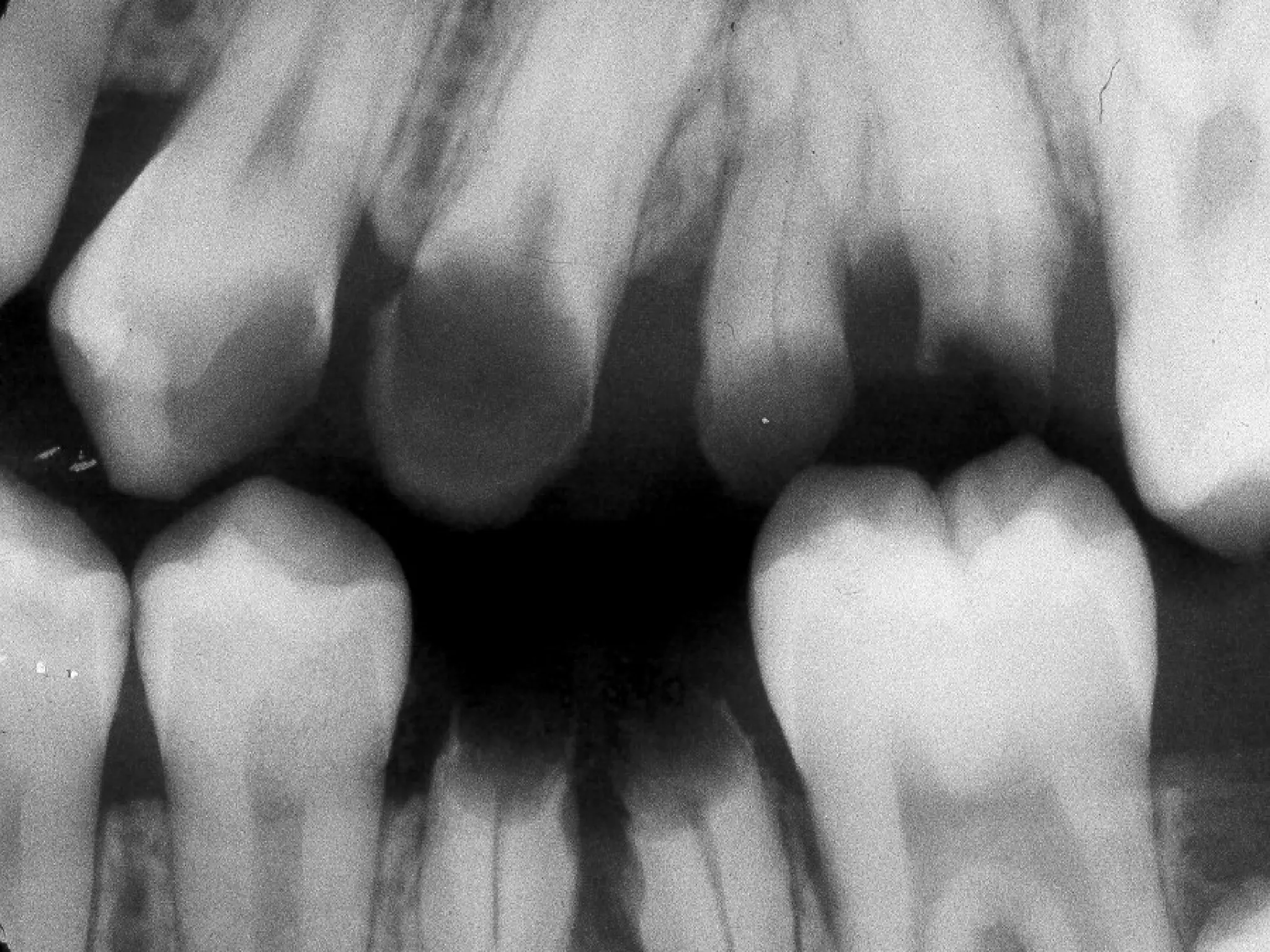


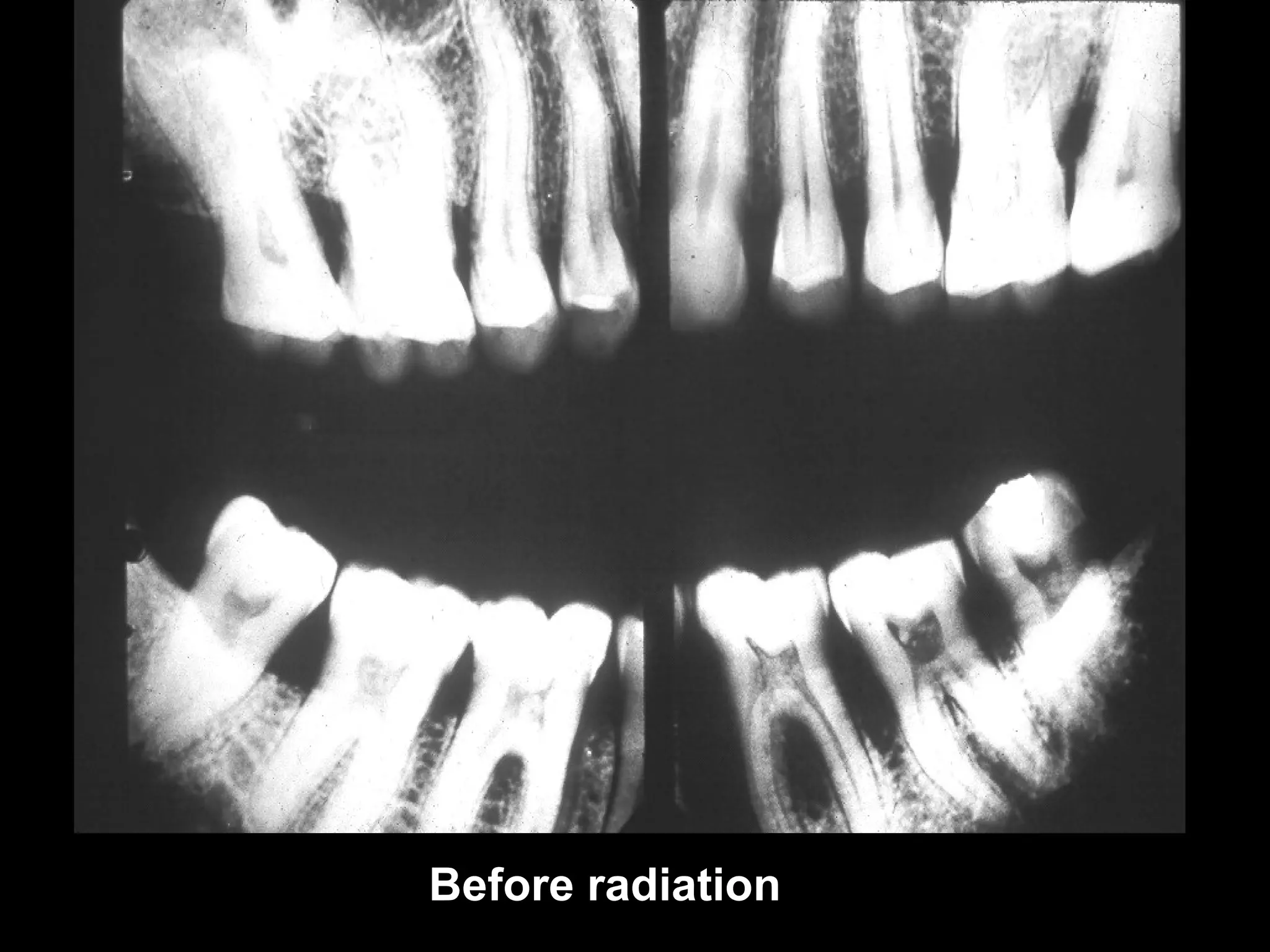




This document describes the radiographic diagnosis of dental caries. It discusses how caries is caused by acid-producing bacteria and can be diagnosed clinically and through radiographs. Bitewing and periapical films are used to identify caries at different angles. Caries appears at different stages from incipient to severe on radiographs. Factors like tooth thickness and x-ray angle affect detectability. Recurrent, root, and radiation-induced caries are also addressed.























































































