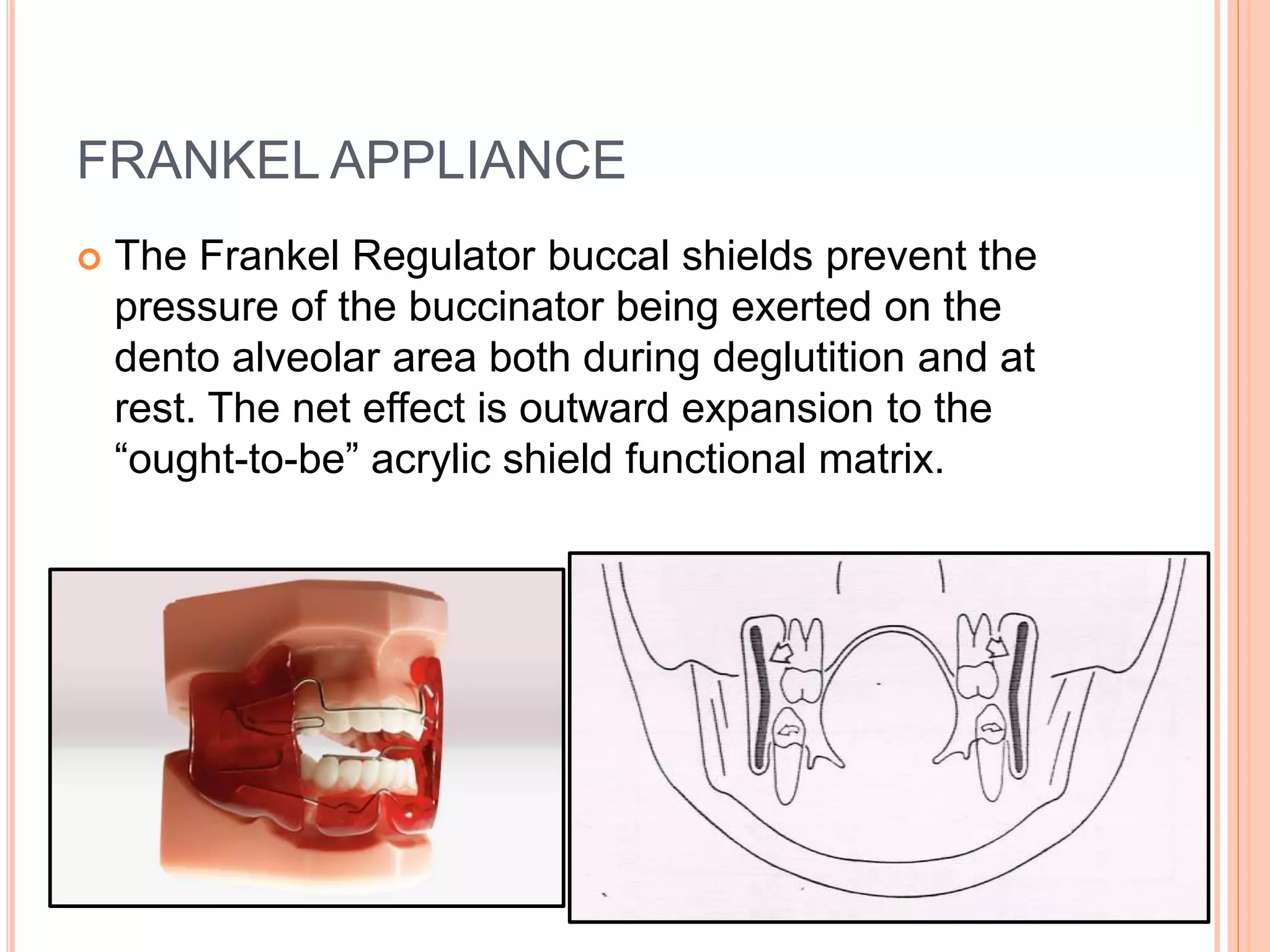
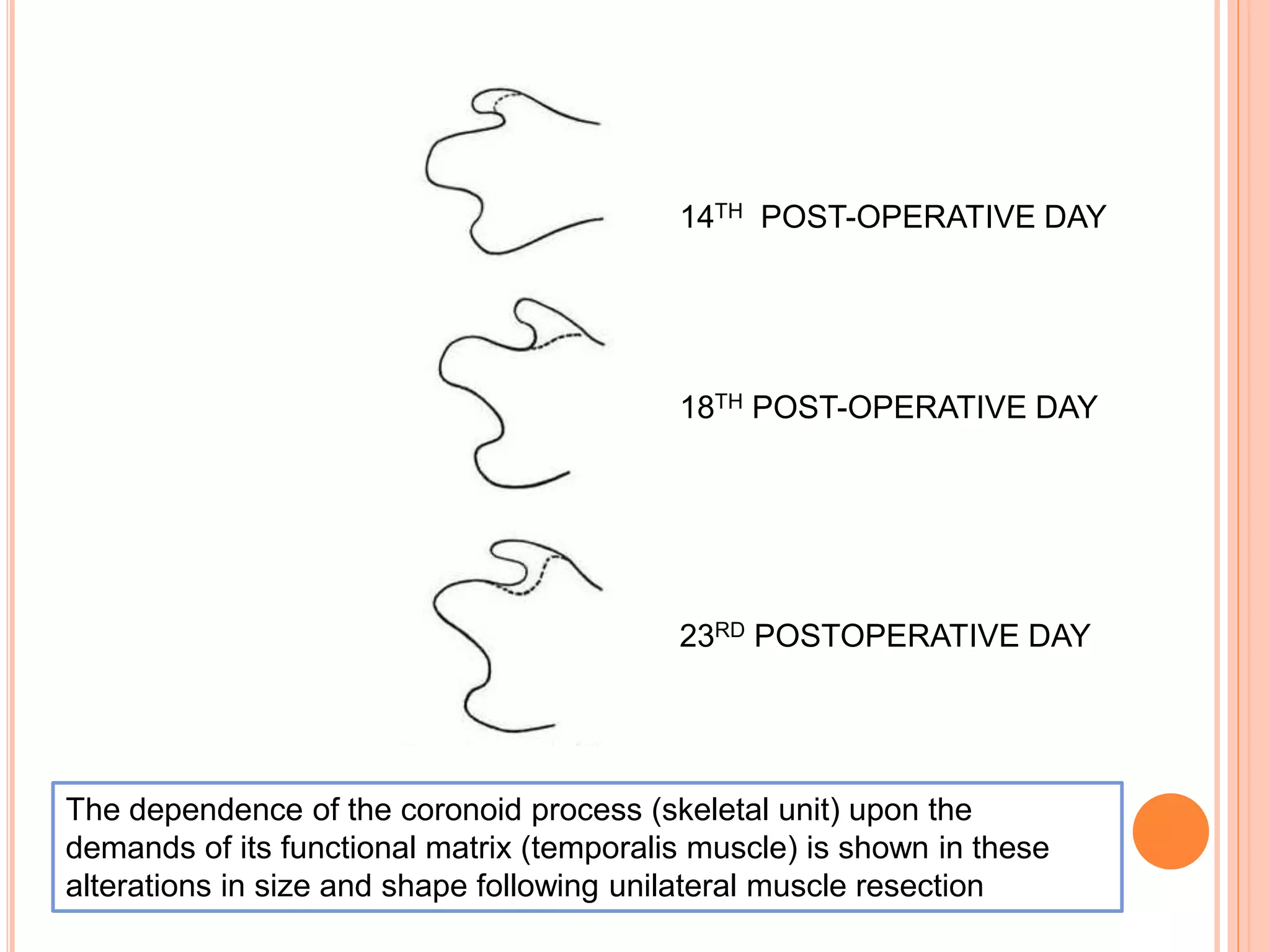
The document summarizes the functional matrix theory of bone growth proposed by Melvin Moss. The theory states that bone growth occurs as a response to functional needs mediated by soft tissues, rather than bones growing independently. Growth involves periosteal matrices altering bone size in response to soft tissue demands, and capsular matrices passively translating bones during expansion. Experiments on rats supported the theory by showing bones altered in size and shape following muscle resection. Clinical implications include functional appliances altering bone growth by changing soft tissue pressures.
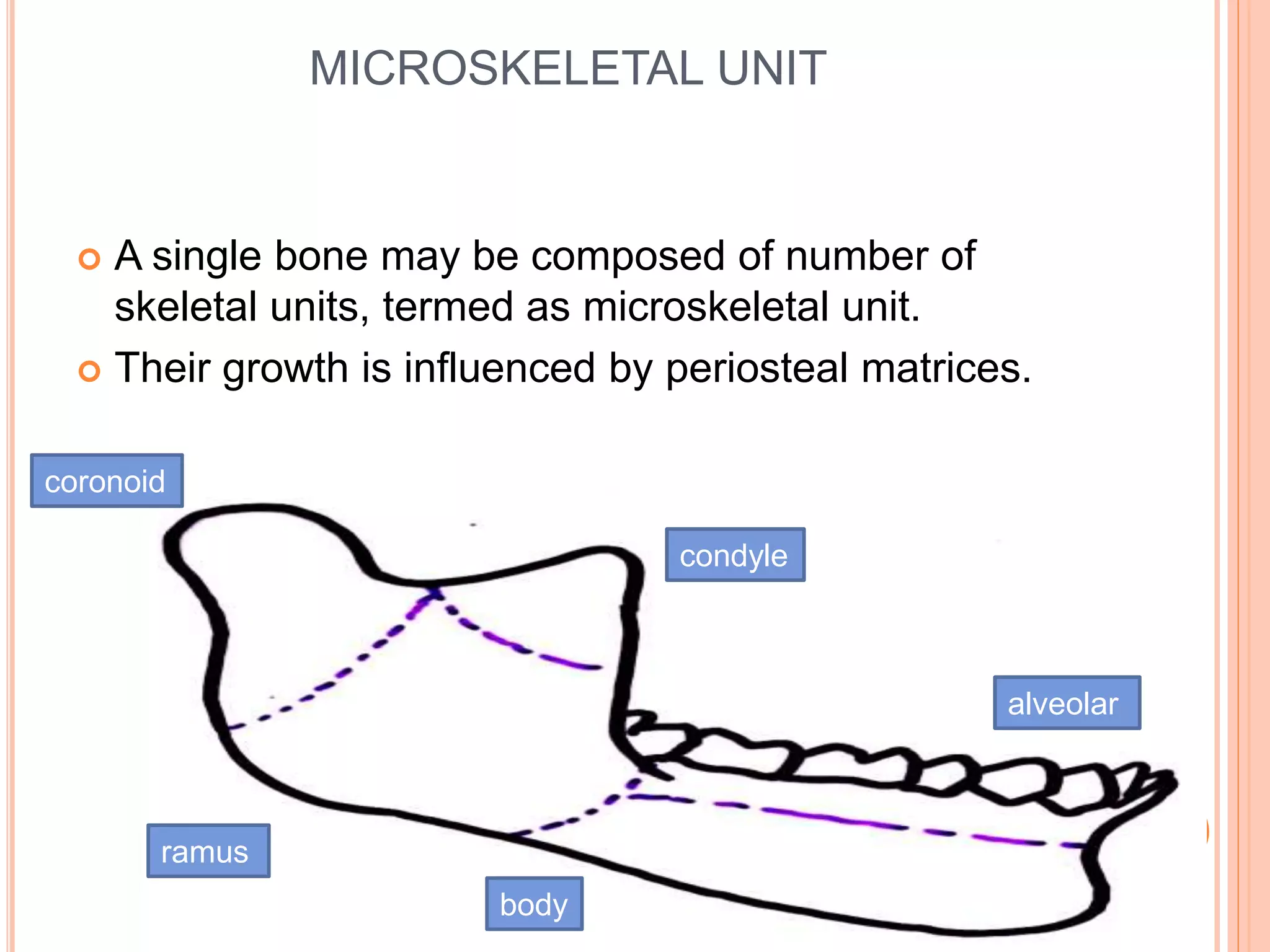
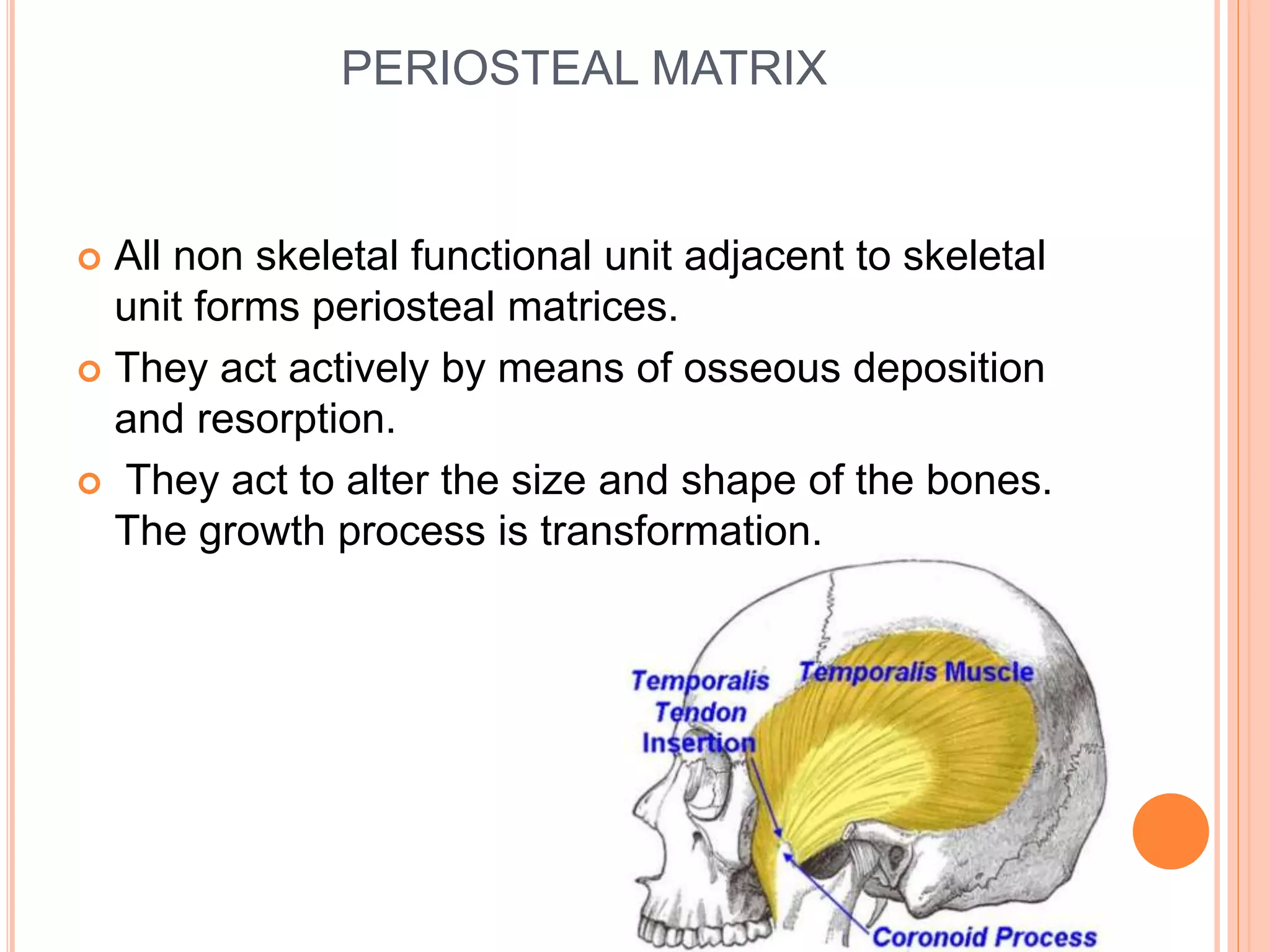
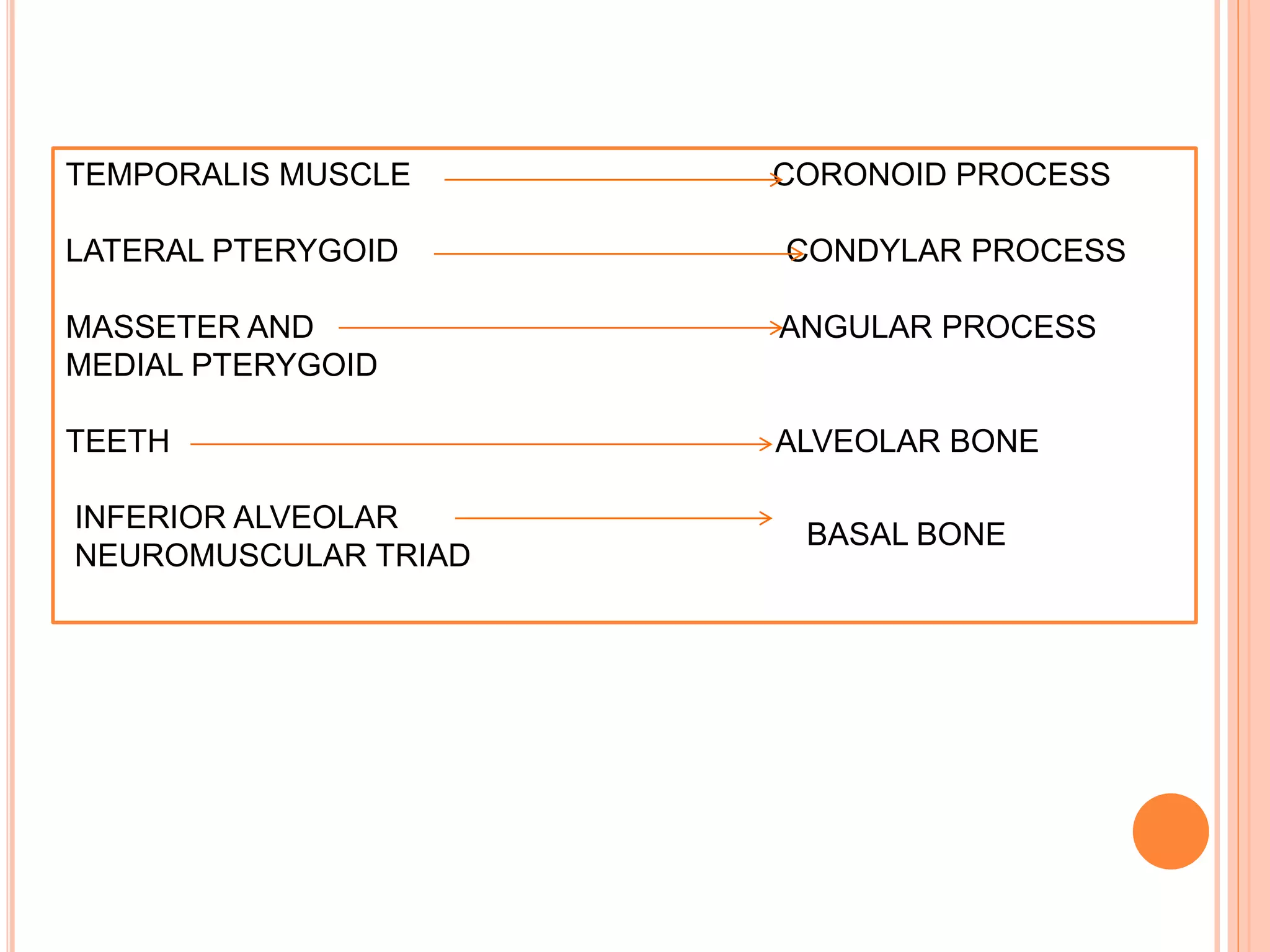
![Periosteal Matrix ------------> Skeletal Unit
[Teeth] [Alveolar Bone]
CLINICALIMPLICATIONS
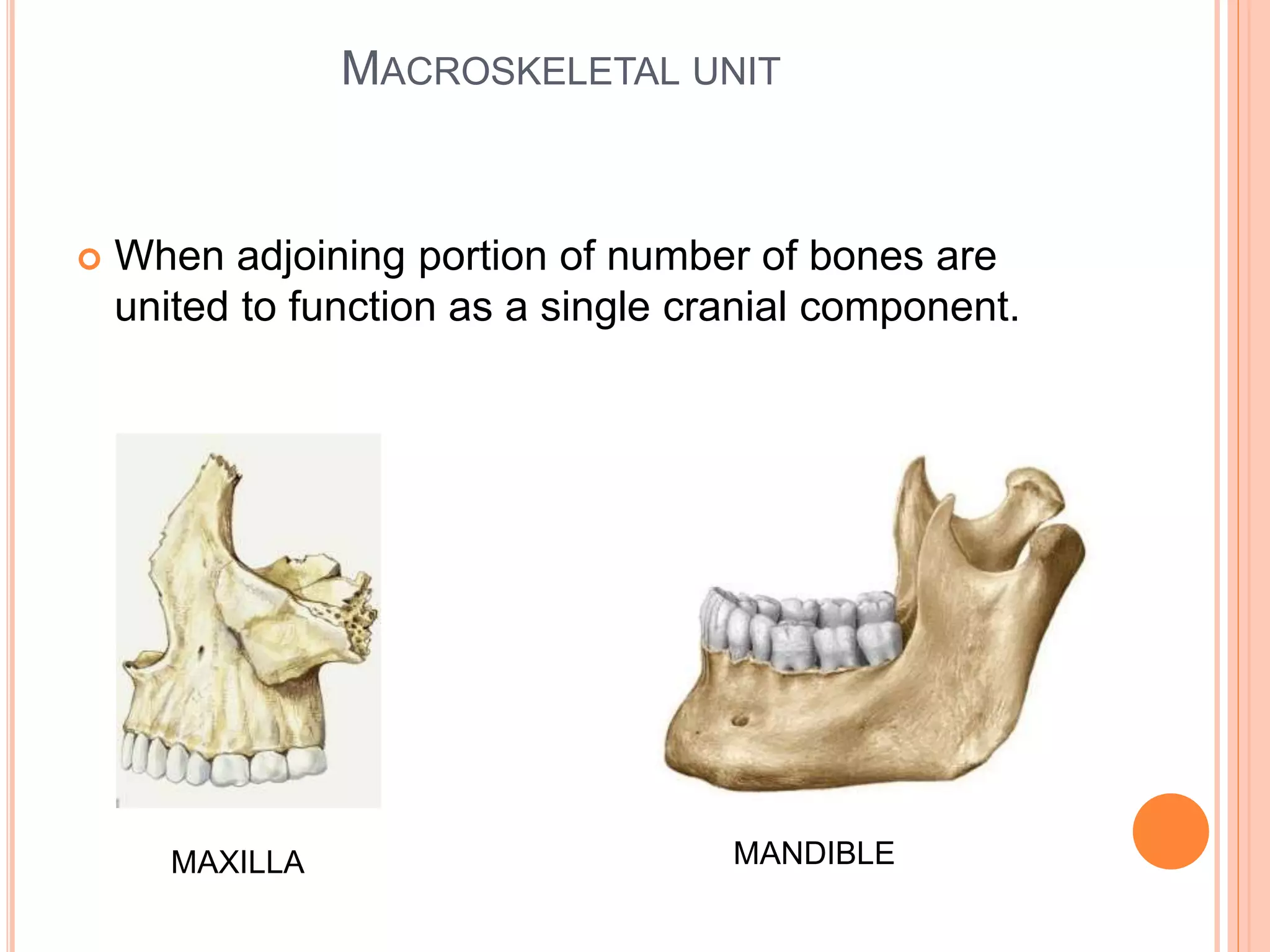
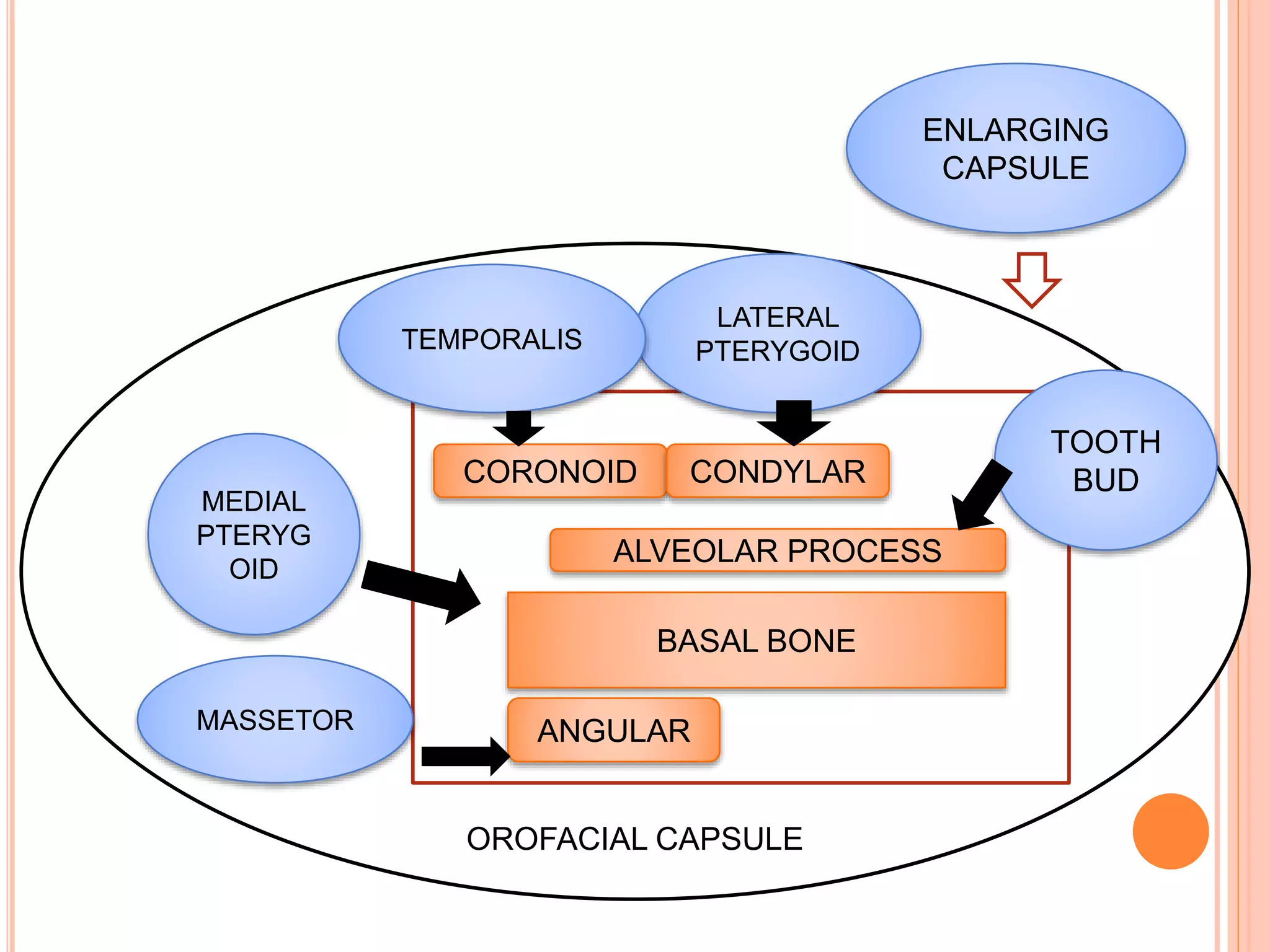
Capsular Matrix -------------> Multiple Skeletal Units
[Functional Appliances] [Jaw Bones]](https://image.slidesharecdn.com/functionalmatrxtheorybyzynuljohn-190405141952/75/Functional-Matrix-Theory-35-2048.jpg)