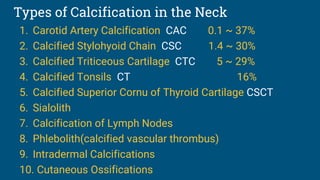
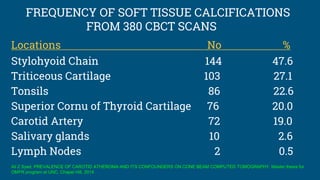
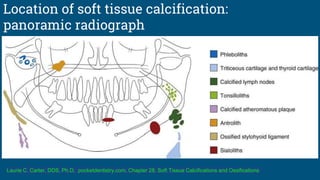
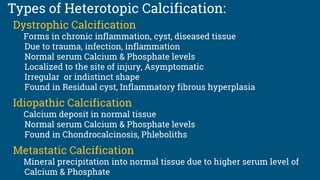


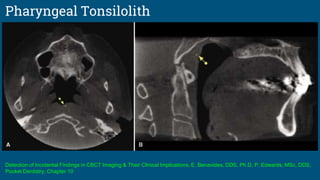
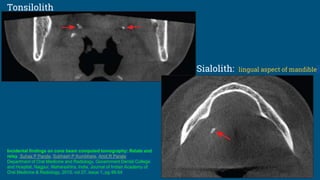



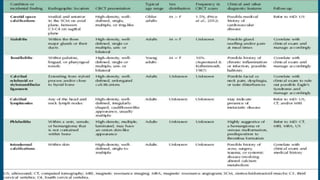
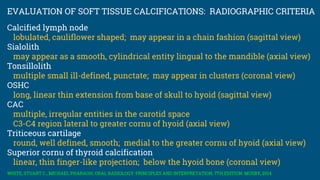


1. The document discusses various types of soft tissue calcification that can be seen in the neck on CBCT imaging, including calcification of the carotid artery, stylohyoid ligament, triticeous cartilage, tonsils, thyroid cartilage, salivary glands, lymph nodes, and veins. 2. It provides the locations, appearances, and frequencies of each type of calcification based on reviews of 380 CBCT scans. Common sites include the stylohyoid ligament, triticeous cartilage, and tonsils. 3. The causes of soft tissue calcification include dystrophic calcification from chronic inflammation or injury, idiopathic calcification, and metastatic calcification from high


































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






