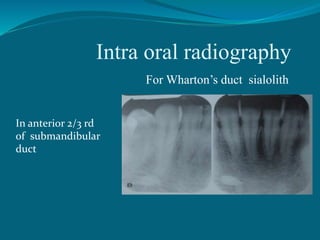
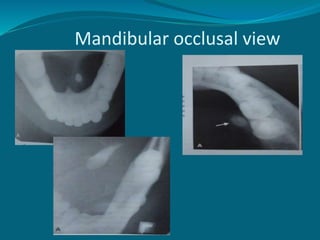
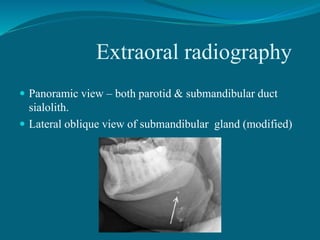
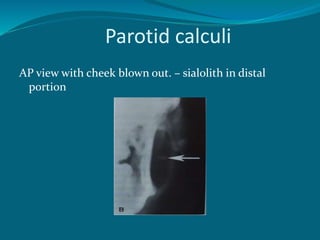
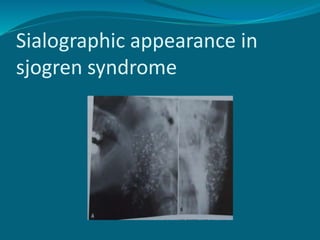
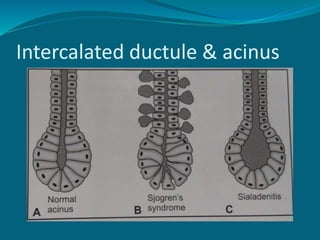
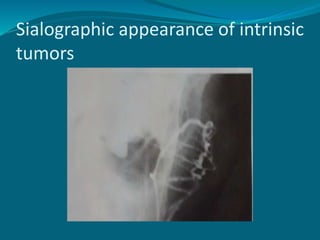
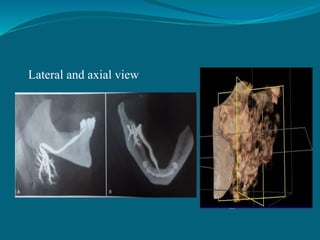
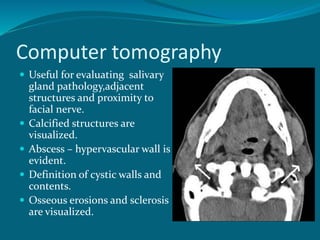
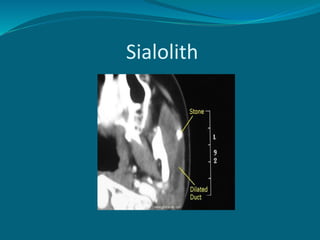
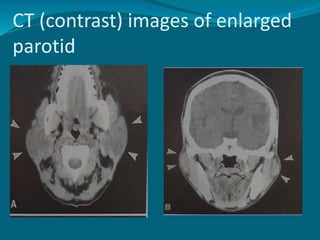
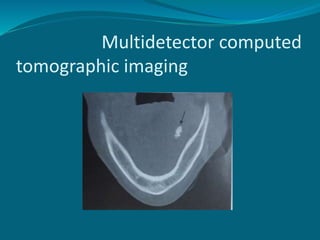
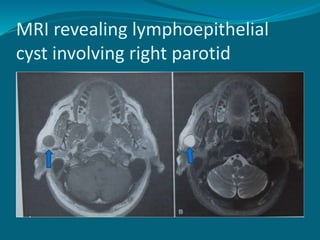
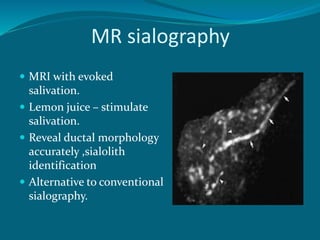
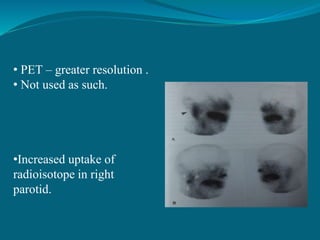
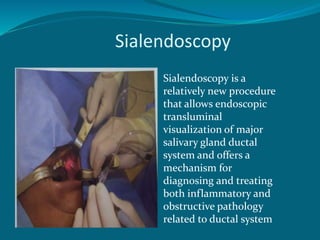
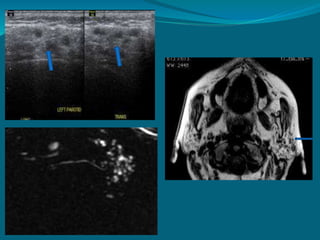
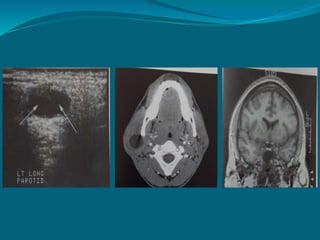
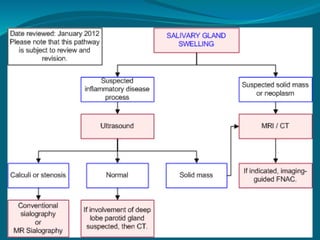
This document discusses the anatomy, imaging, and clinical evaluation of the salivary glands. It describes the major and minor salivary glands and lists common salivary gland complaints such as sialolithiasis, infection, Sjogren's syndrome, and tumors. Imaging modalities for evaluating salivary glands are discussed, including intraoral radiography, sialography, ultrasound, CT, MRI, scintigraphy, and sialendoscopy. The document provides examples of how various salivary gland pathologies appear on different imaging tests.