Downloaded 222 times

































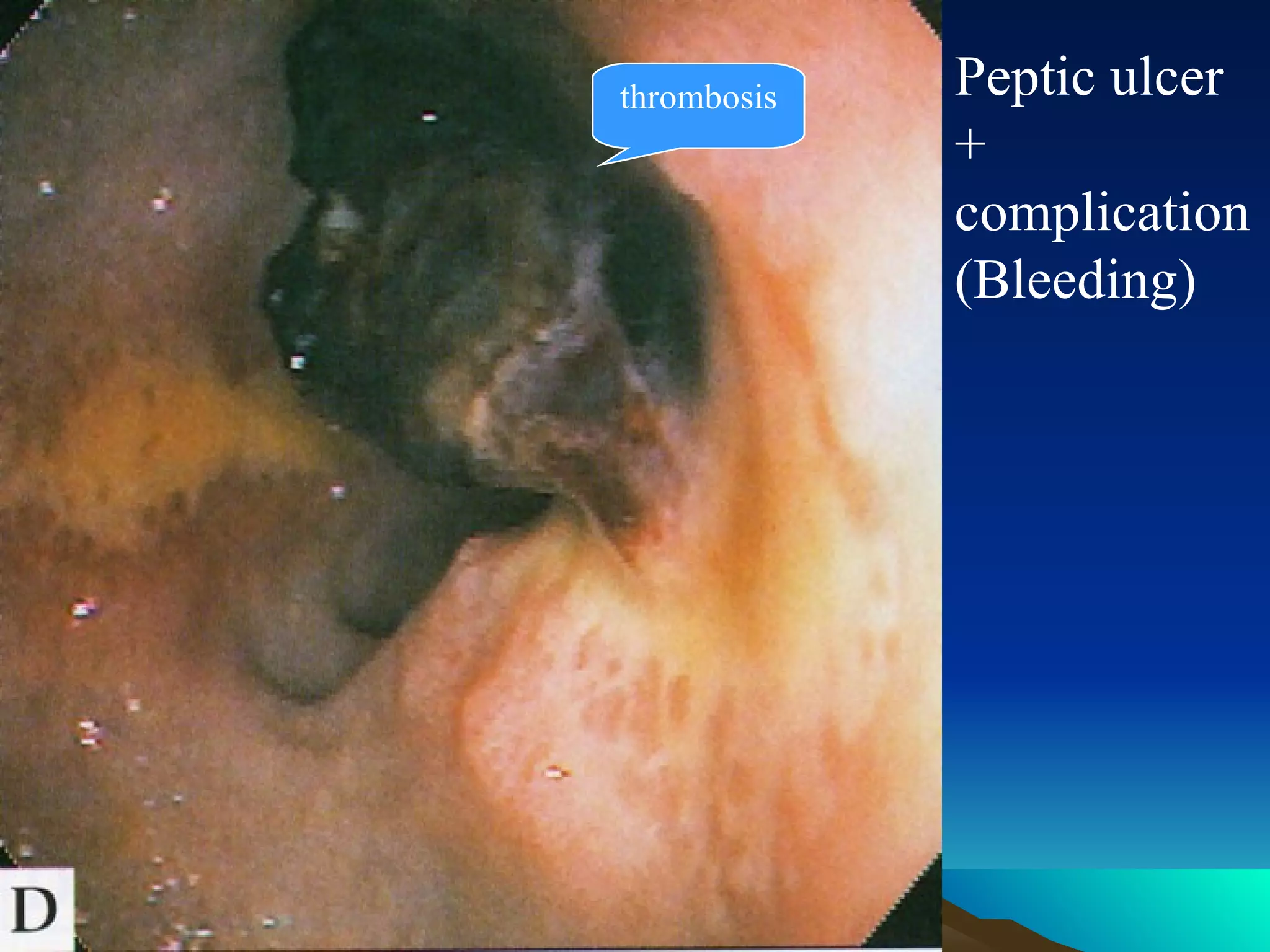












This document describes a case of a 75-year-old man admitted to the ICU with respiratory failure, pneumonia, and stress ulcer syndrome. It provides details on his medical history, symptoms, lab results, diagnoses, and proposed treatment. It then discusses stress ulcer syndrome in more detail, covering topics like definition, etiology, pathogenesis, risk factors, diagnosis, treatment principles including cytoprotection, acid suppression, and enteral feeding, and prophylaxis for at-risk patients. The key point is that stress ulcers result from mucosal ischemia in critically ill patients and treating the underlying condition along with gastric acid suppression and cytoprotection can help prevent bleeding complications.























































































