Download as PDF, PPTX
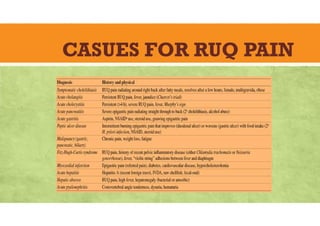
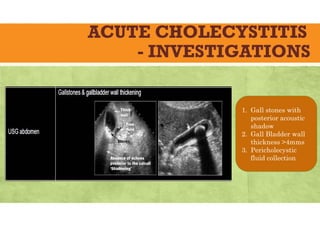
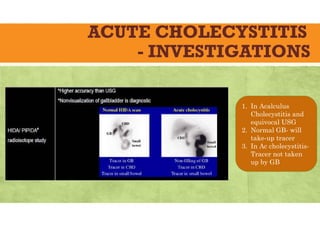
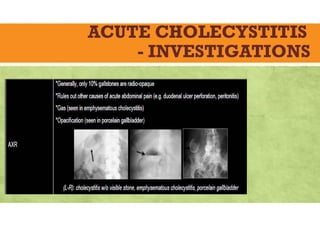
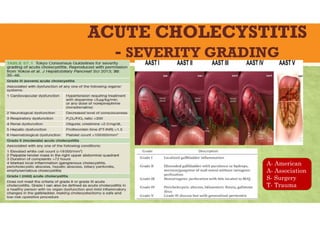
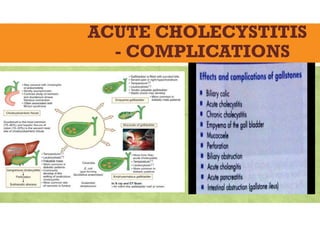
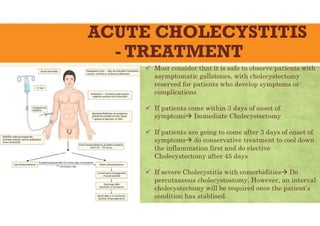
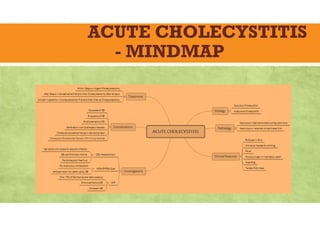
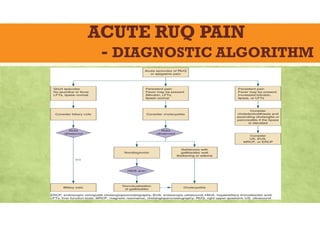


The document provides a comprehensive overview of acute cholecystitis, detailing its causes, epidemiology, etiology, pathology, clinical features, investigations, complications, and treatment. It emphasizes the significance of gallstones and their relation to the condition, along with risk factors and management strategies, including the importance of timely surgical intervention. Clinical features and diagnostic approaches are also outlined to aid in the assessment and treatment of patients with acute cholecystitis.























































































