Downloaded 1,005 times

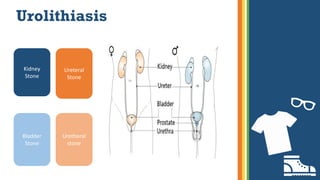

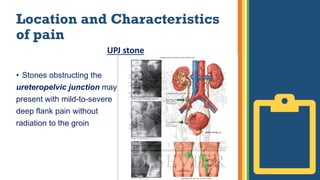
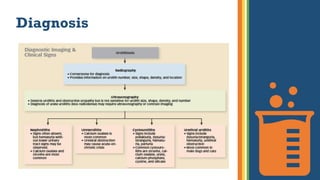


Urolithiasis, or the formation of urinary stones, is a common condition impacting millions and costing the U.S. healthcare system over $2 billion annually. Factors influencing stone formation include age, sex, diet, and familial history, with symptoms varying from severe pain to asymptomatic presentations. Diagnosis involves physical examination, imaging, and laboratory tests, followed by management strategies that include pain relief, medical expulsive therapy, and surgical options when necessary.



































































