Downloaded 841 times

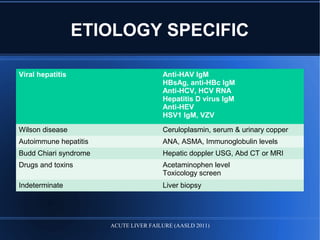
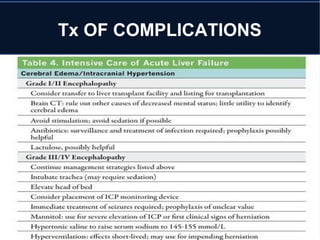
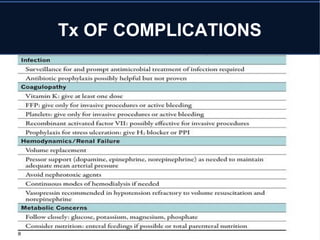
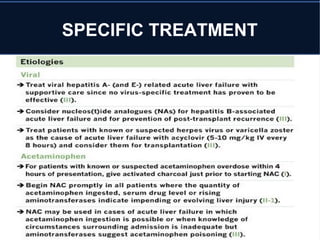
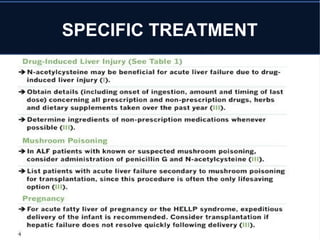

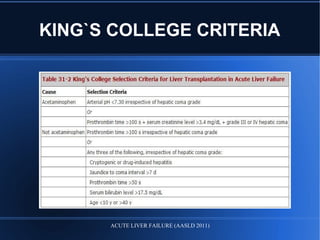

Acute liver failure (ALF) is a rare condition defined as a rapid deterioration of liver function resulting in altered mental status and coagulopathy in individuals without pre-existing liver disease within 26 weeks. It carries a high mortality and often affects young persons. The document discusses the causes, clinical presentation, complications, diagnosis, and management of ALF including supportive care, specific treatments, liver transplantation, and prognosis.

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















