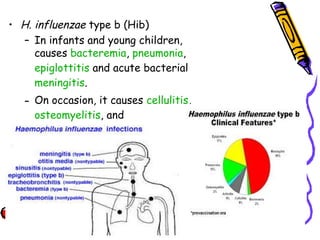
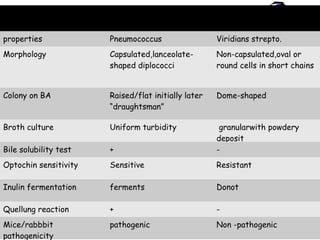
Streptococcus pneumoniae and Hemophilus influenzae are common causes of pneumonia and other respiratory infections. S. pneumoniae is a gram-positive diplococcus that causes pneumonia, otitis media, bacteremia and meningitis, especially in children. H. influenzae is a gram-negative coccobacillus found in the nasopharynx that can cause pneumonia, epiglottitis, bacteremia and meningitis, particularly in young children from encapsulated strains like type b. Both bacteria require special growth factors and are diagnosed through culture, staining, and serological testing. Effective vaccines exist for prevention of disease caused by these pathogens.



































![Haemophilus influenzae
• gram-negative coccobacillus(short rod) and long
filamentous form in CSF in meningitis.
• 0.2 to 0.3 to 0.5 to 0.8 um
• Nonmotile, nonsporing pleomorphic
• Oxidase positive
• aerobic and facultative anaerobe.
• In vitro growth requires accessory growth factors,
including “X” factor (hemin) and “V” factor
(nicotinamide adenine dinucleotide [NAD]).
• Chocolate agar media are used for isolation. H.
influenzae will generally not grow on blood agar, which
lacks NAD.](https://image.slidesharecdn.com/streptococcuspneumoniaembbs-160120132010/85/Streptococcus-pneumoniae-mbbs-37-320.jpg)