Downloaded 755 times







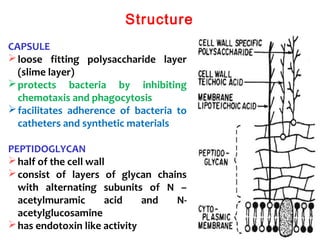



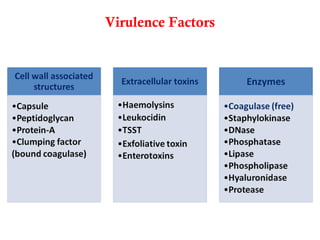











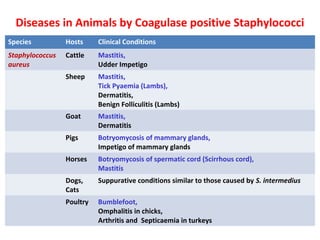








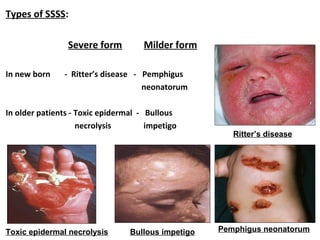




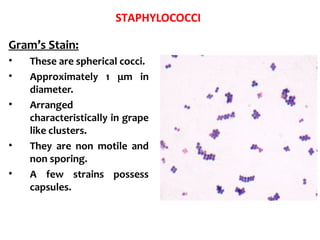









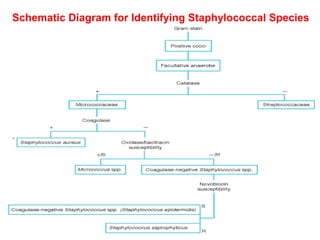


This document provides information on the genus Staphylococcus. It discusses the morphology, classification, virulence factors, and diseases caused by Staphylococcus species. Some key points include: - Staphylococcus is a genus of gram-positive bacteria that forms grapelike clusters and includes major human pathogens. - Important virulence factors include toxins like alpha toxin, enterotoxins, and exfoliative toxins. Enzymes and surface proteins also contribute to pathogenesis. - Major diseases caused by coagulase-positive Staphylococcus include mastitis, tick pyemia, exudative dermatitis, and botryomycosis in various animal