
































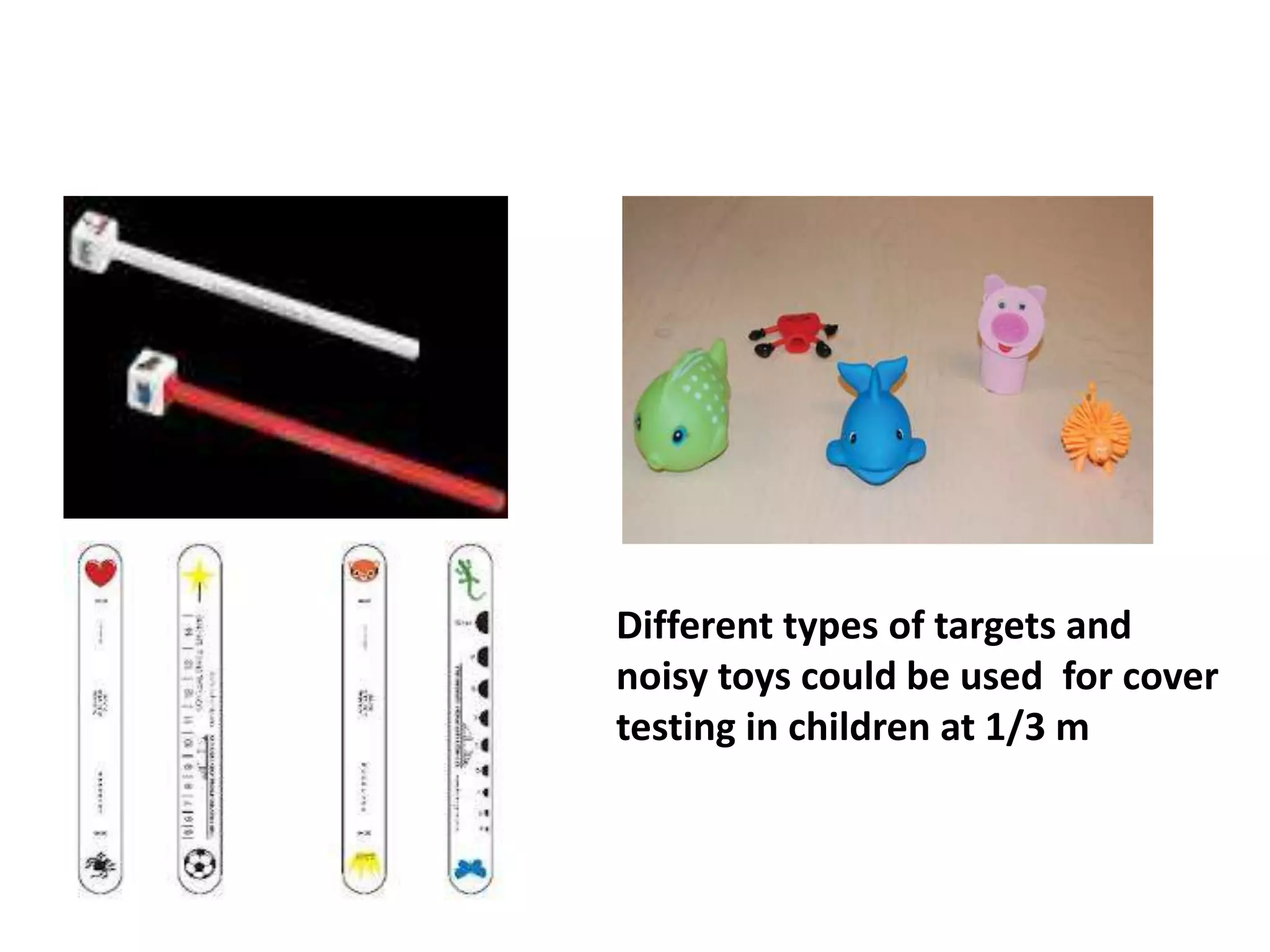


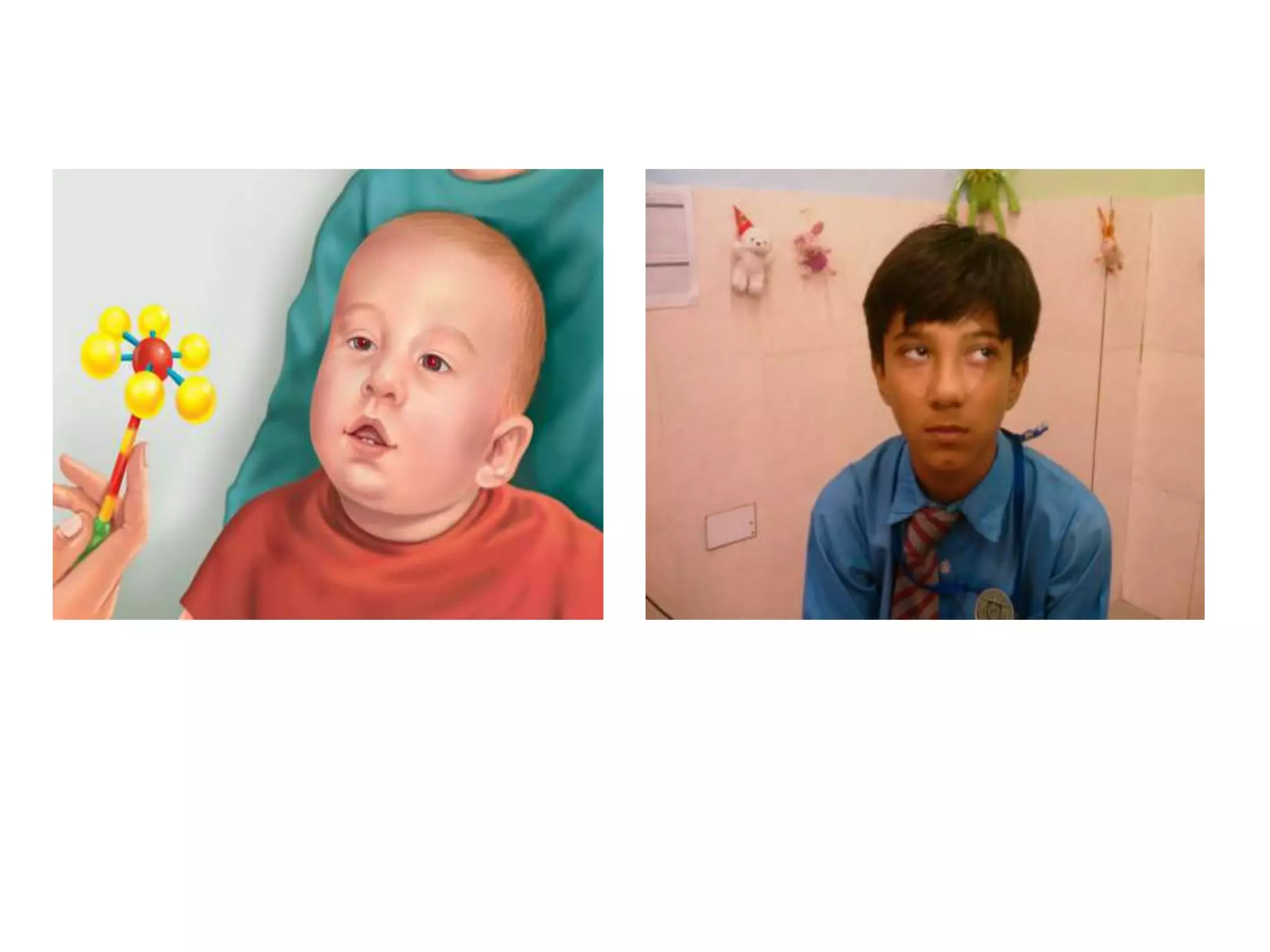

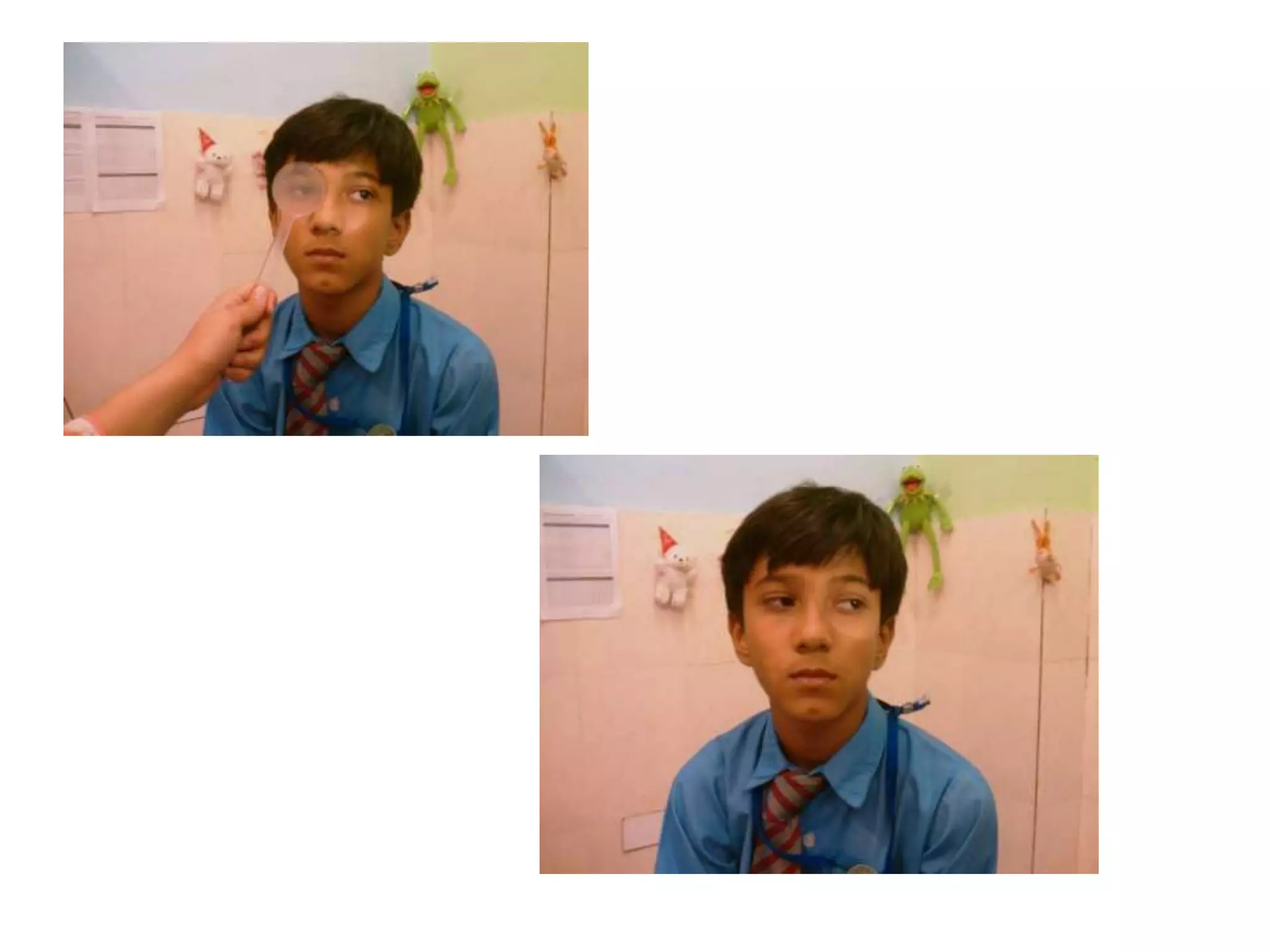











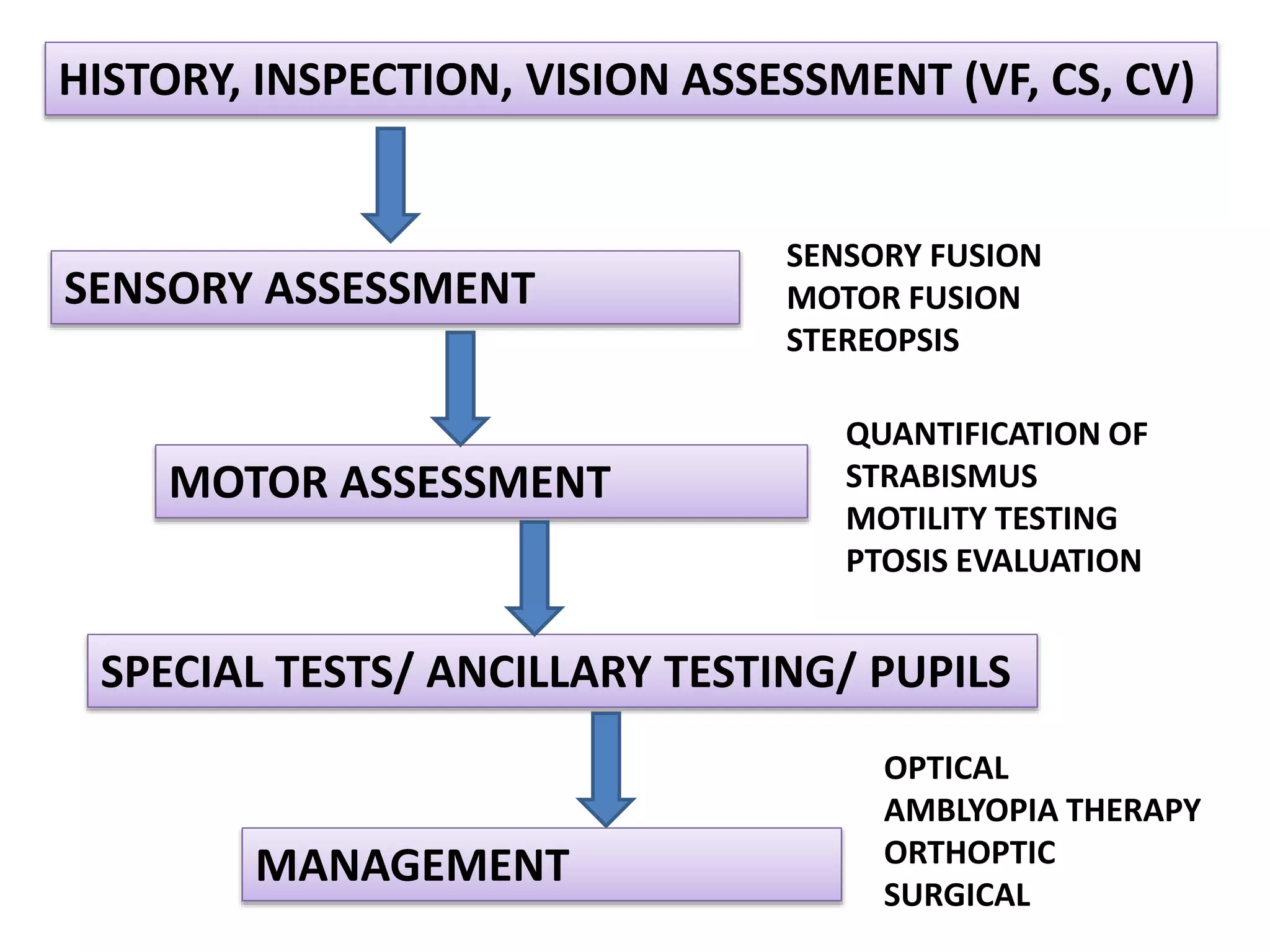


This document provides an overview of assessing strabismus in children. It discusses classifying strabismus based on age, taking a thorough patient history, performing a visual assessment including visual acuity and binocularity tests, and conducting a sensory and motor assessment of eye alignment and eye movement. The motor assessment involves tests like cover testing, versions, ductions, and special tests like vestibular eye movements. Taking this comprehensive approach allows for correctly diagnosing the type and extent of strabismus and determining appropriate management options.















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







