Downloaded 550 times







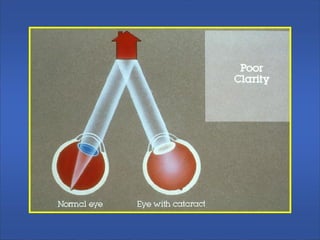















































This document discusses amblyopia, including its classification, etiology, and diagnosis. It defines amblyopia as a decrease in visual acuity caused by pattern vision deprivation or abnormal binocular interaction that cannot be corrected by optical or surgical means. Amblyopia can be functional, resulting from stimulus deprivation, strabismus, refractive errors, or anisometropia, or organic, caused by retinal diseases, nutritional deficiencies, or toxins. The document covers various types of amblyopia in detail and discusses methods for detecting, investigating, and determining the prognosis of amblyopia.























































































