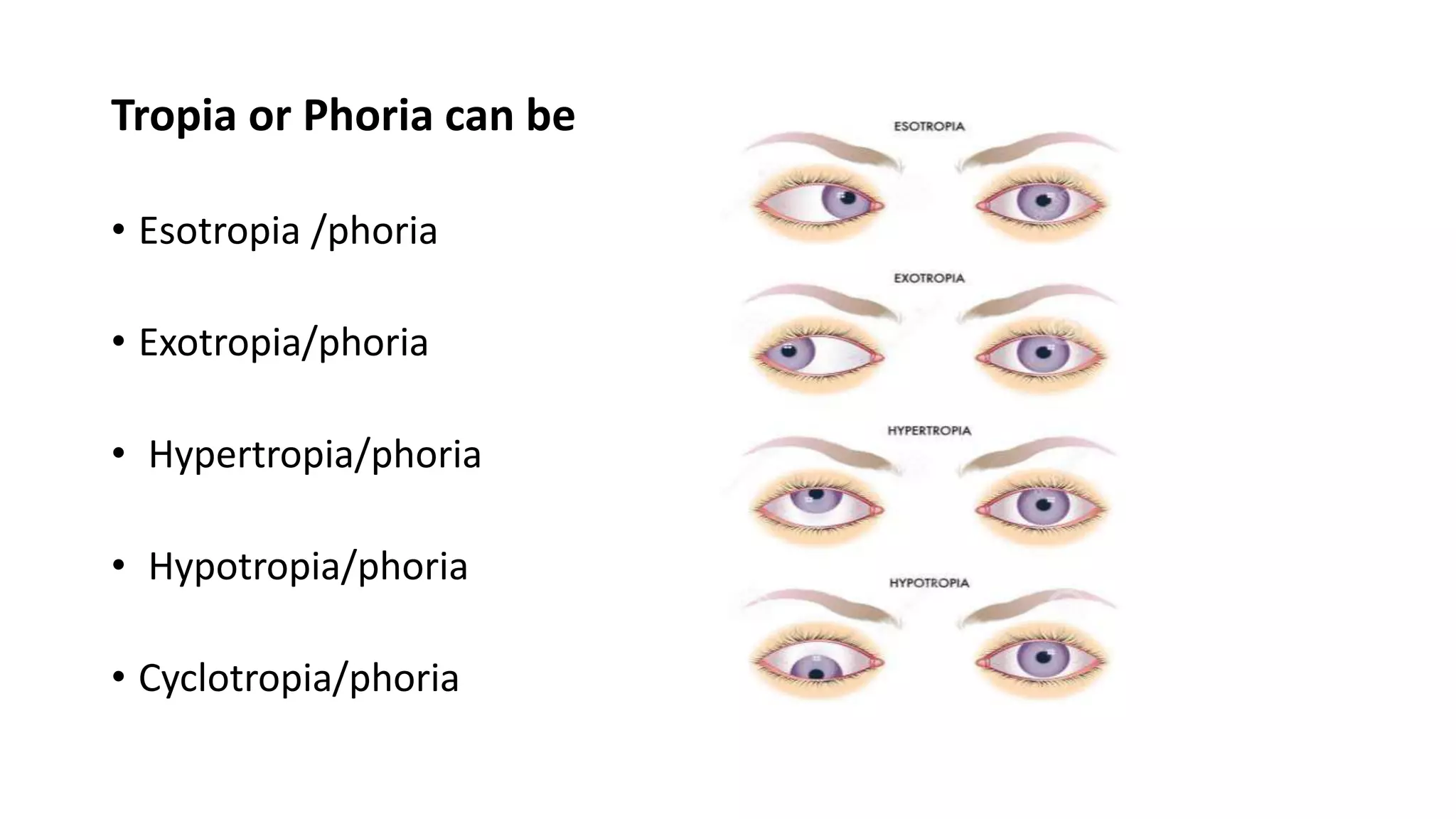
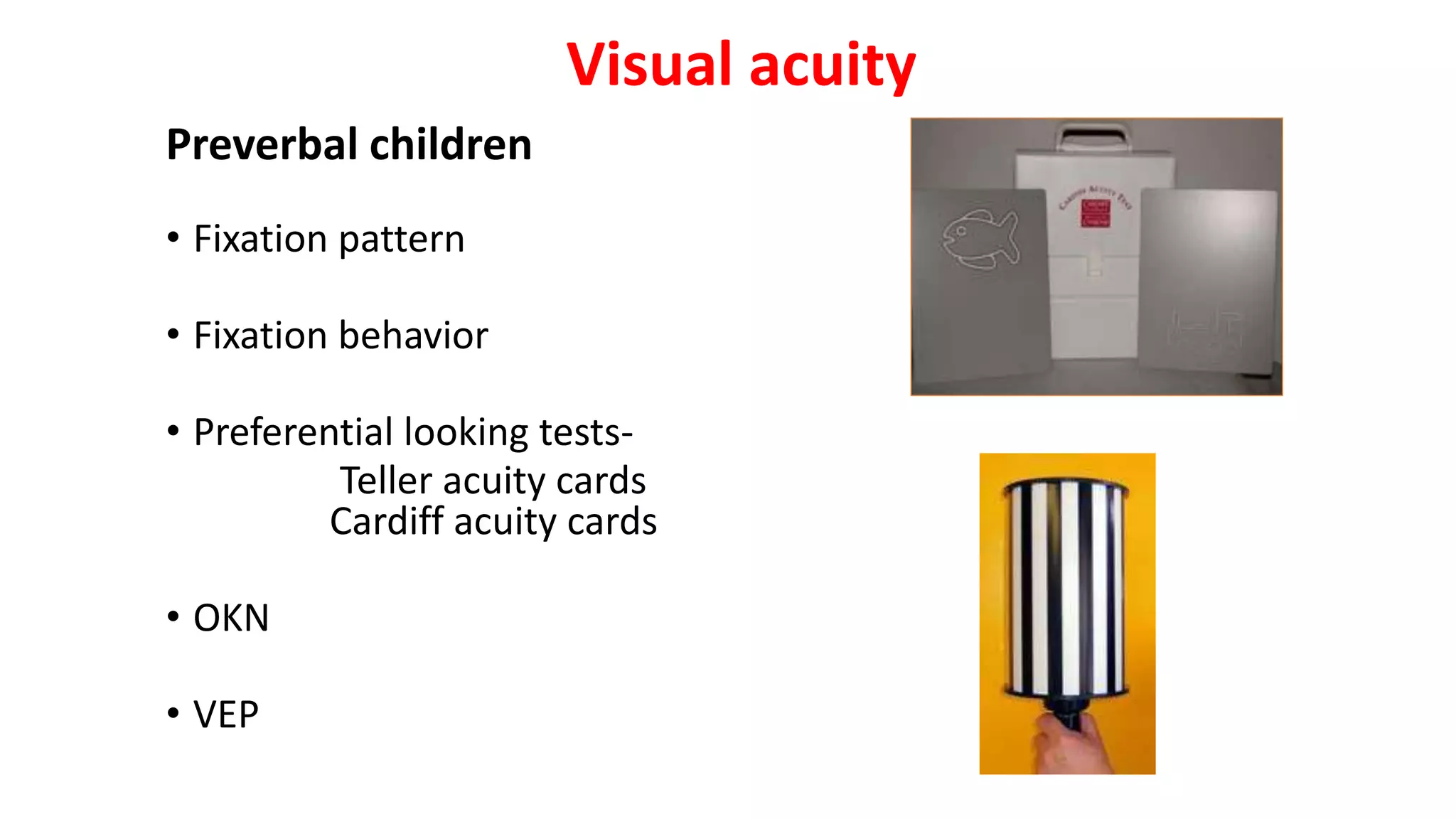
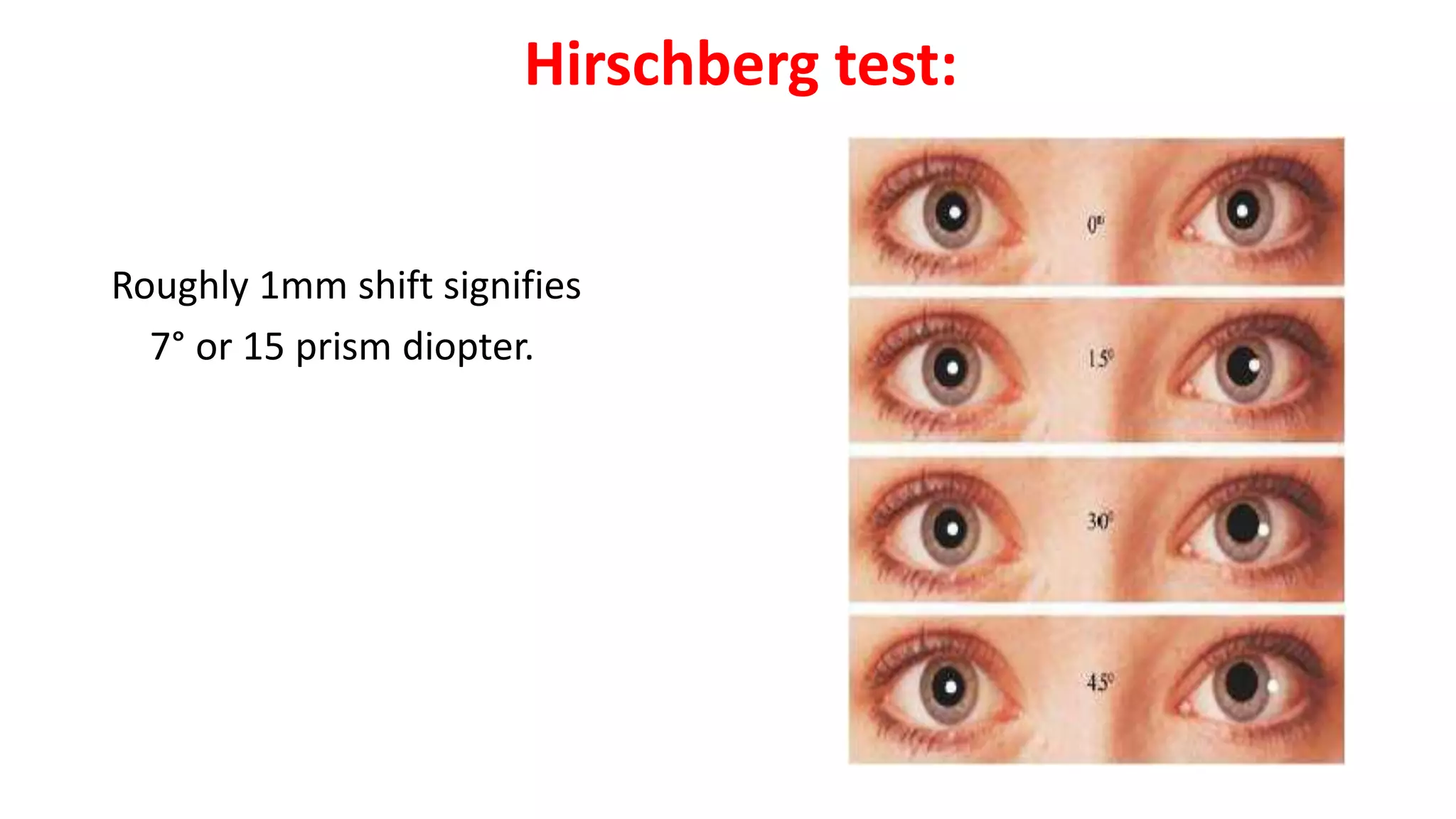
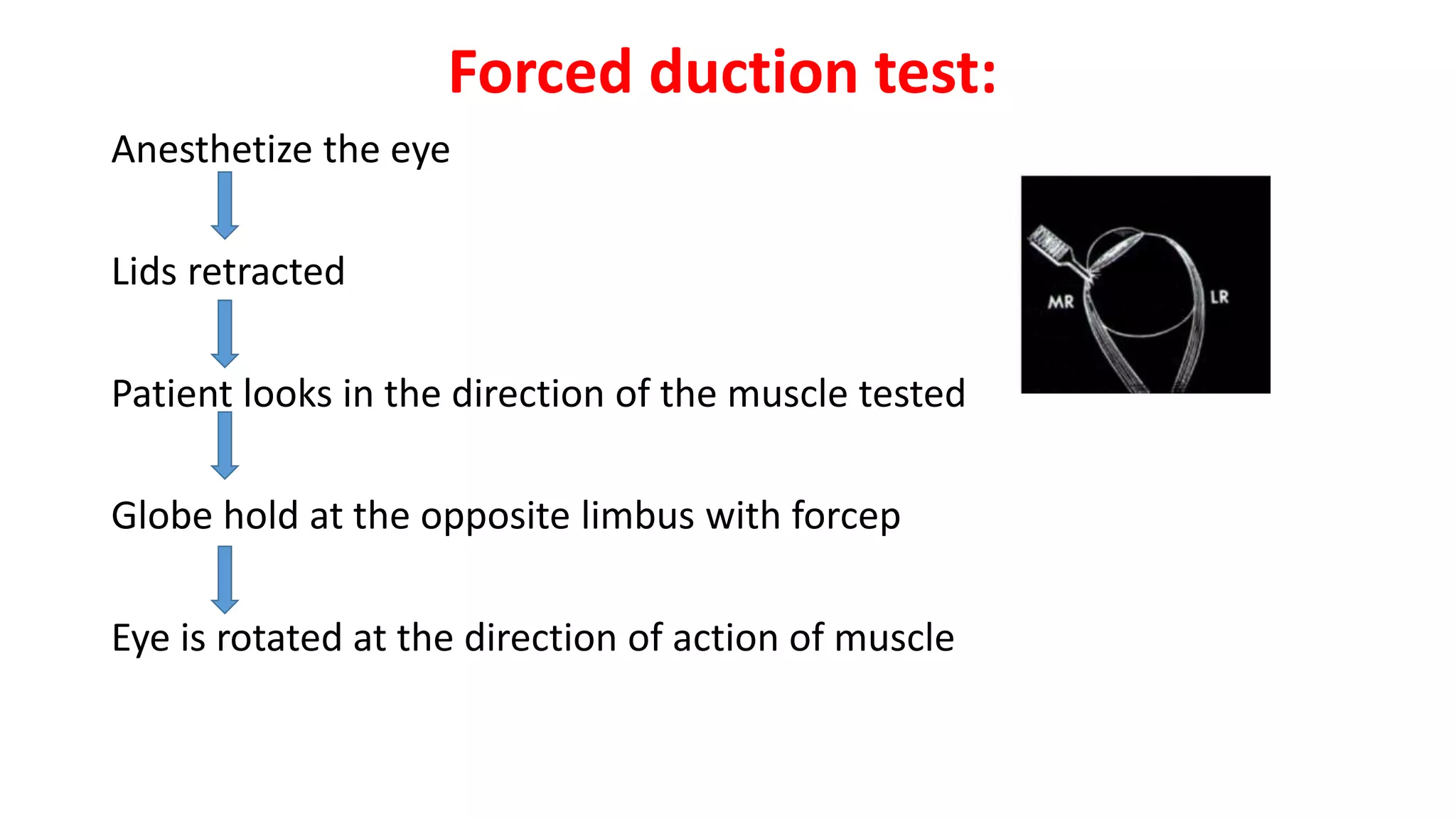
Strabismus is a condition where the visual axes of the two eyes do not align at the point of fixation. It can be comitant, where the misalignment is consistent in all directions of gaze, or incomitant, where the deviation varies with gaze direction. A thorough assessment of strabismus involves testing visual acuity, refractive error, ocular alignment with cover tests and prism bars, ocular motility, binocular vision, and specialized tests like forced duction testing. The evaluation aims to determine the type and size of strabismus, assess binocular function, and identify any underlying causes.