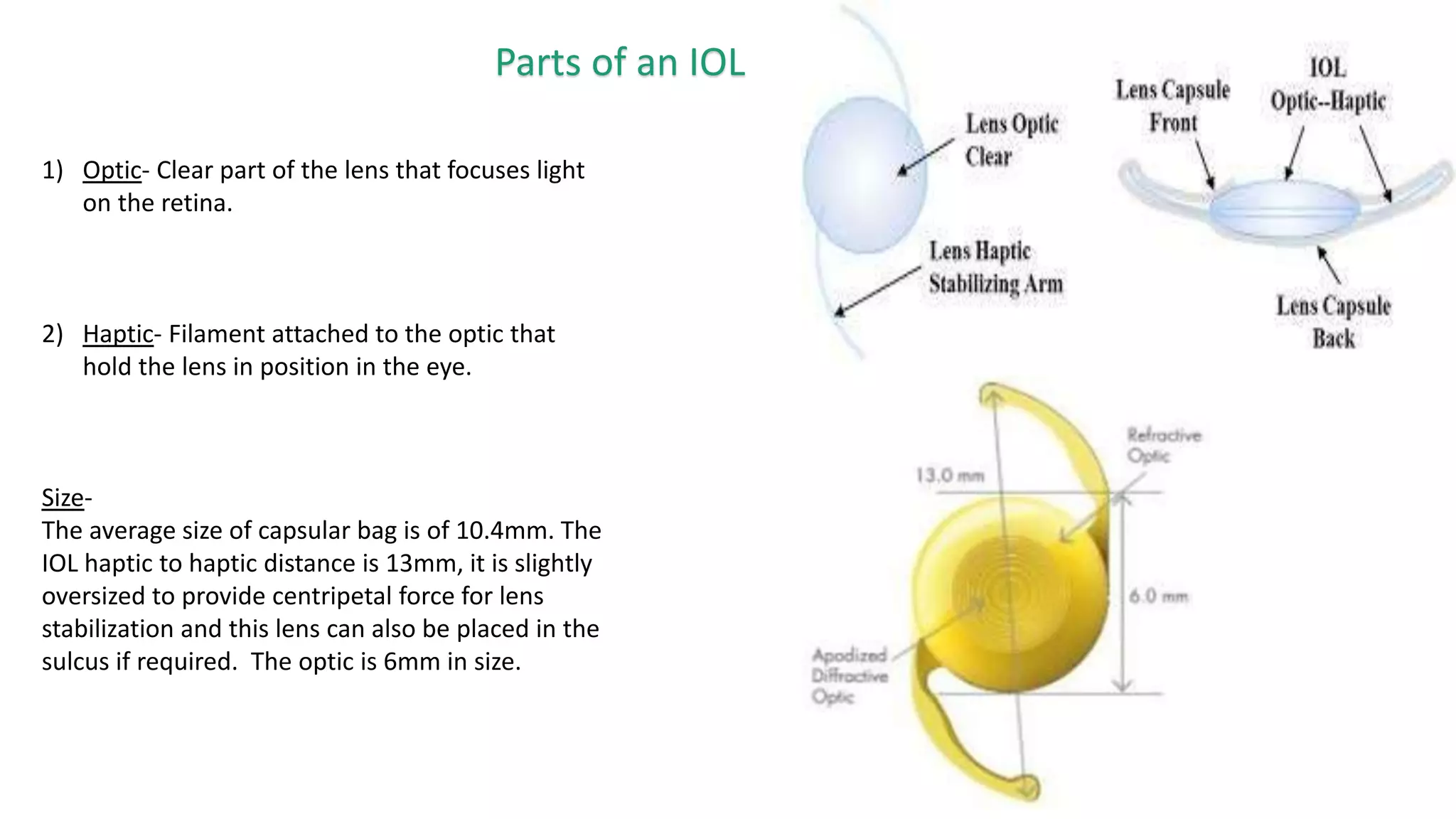
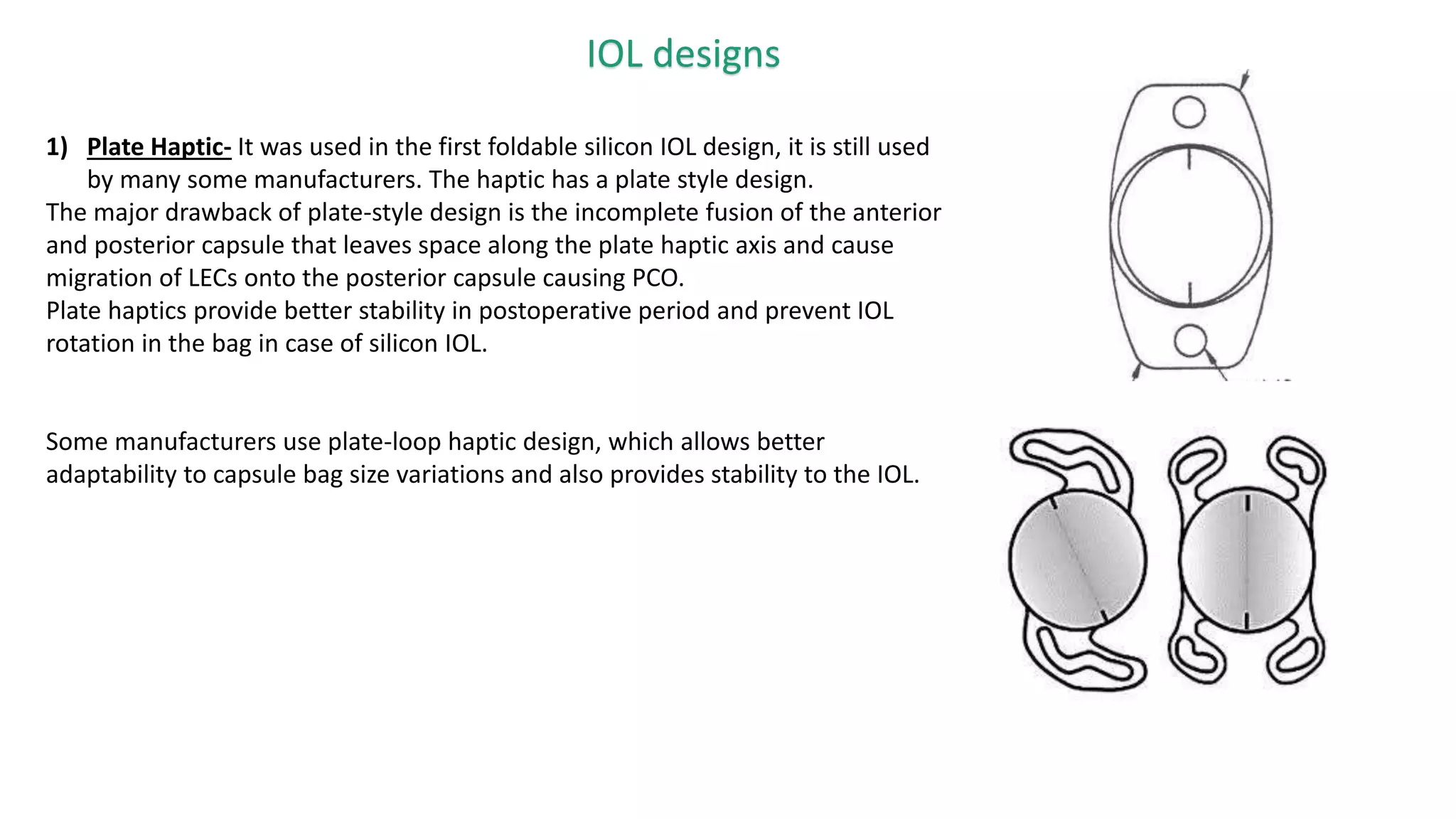
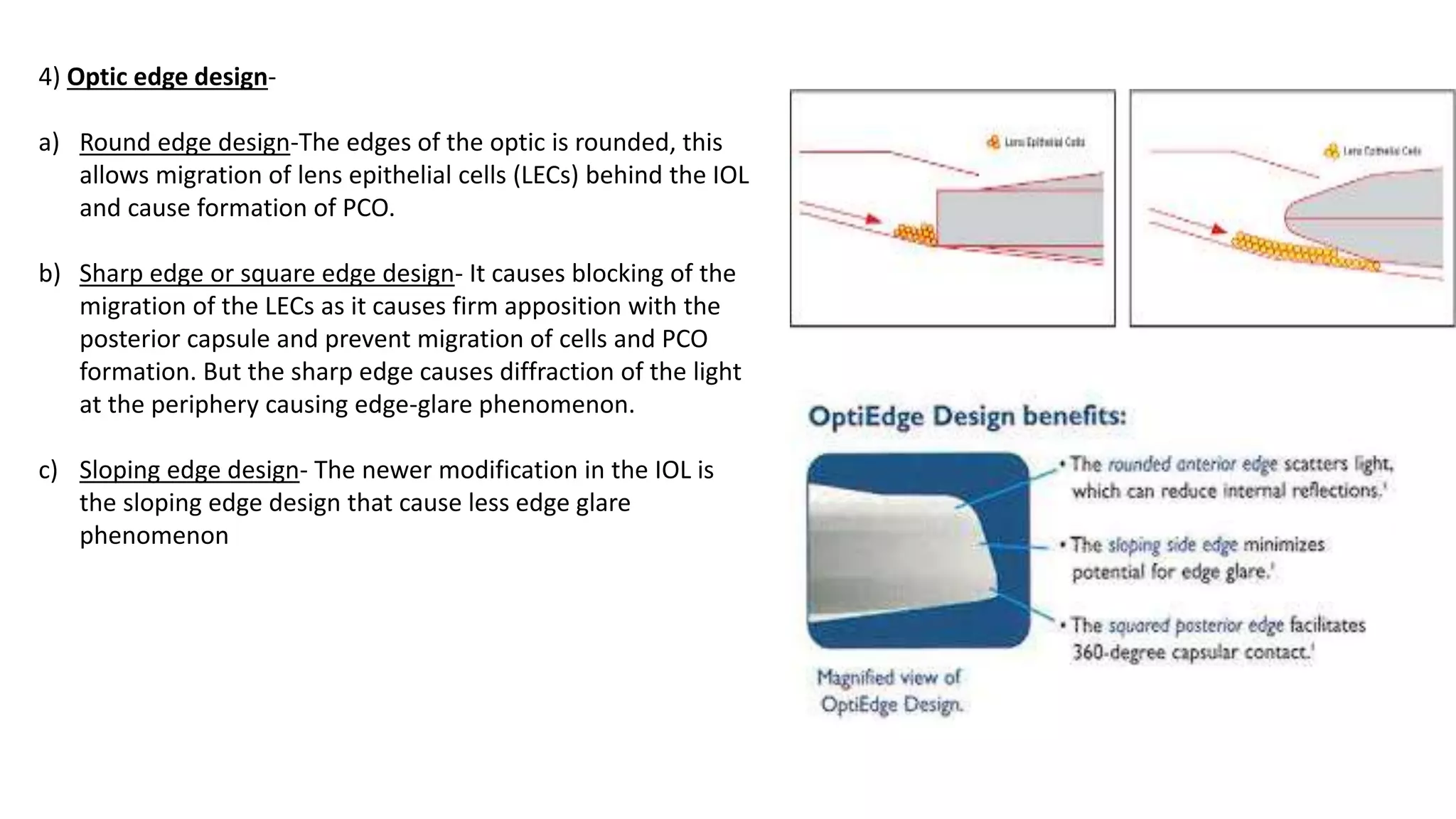
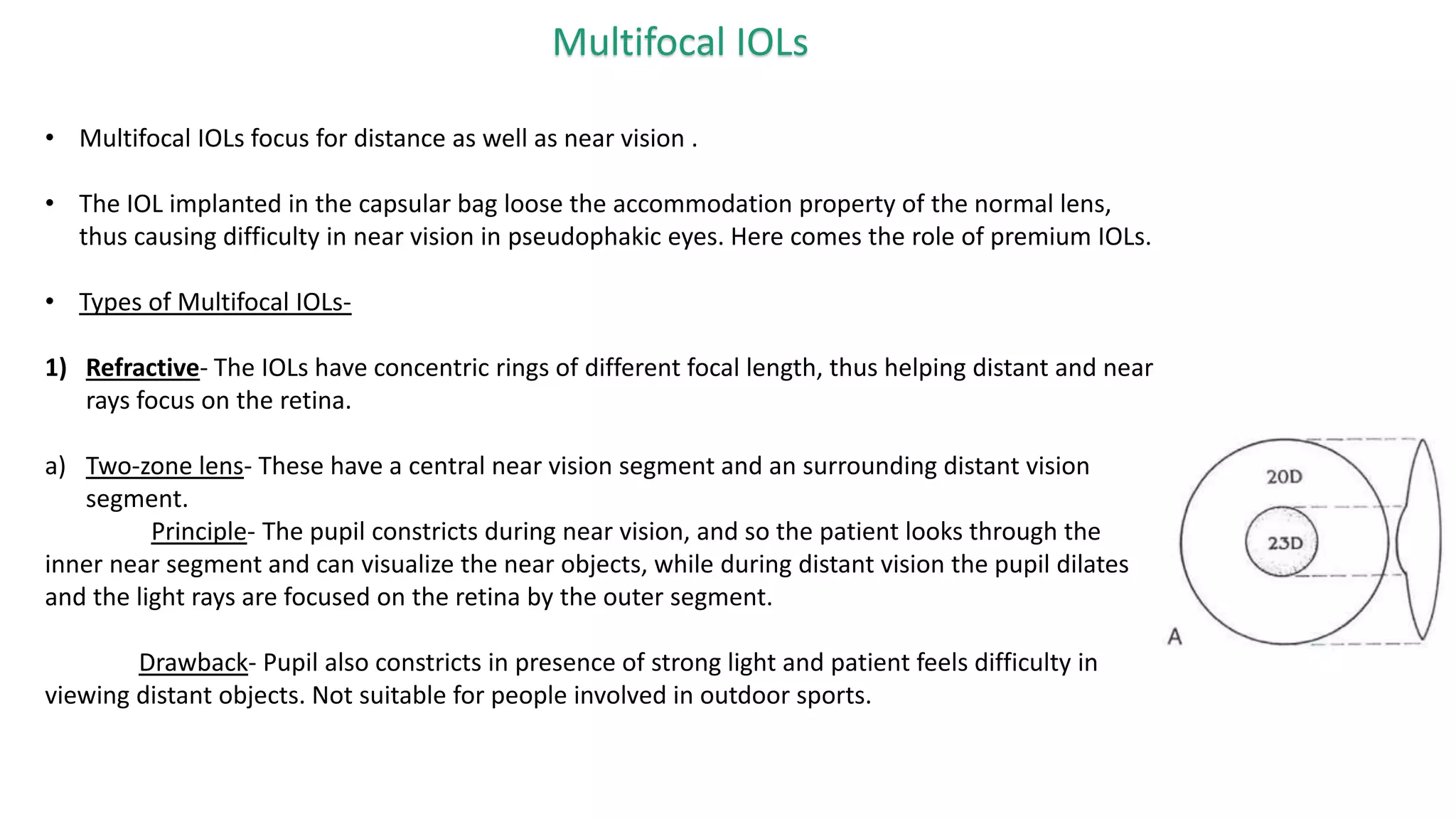
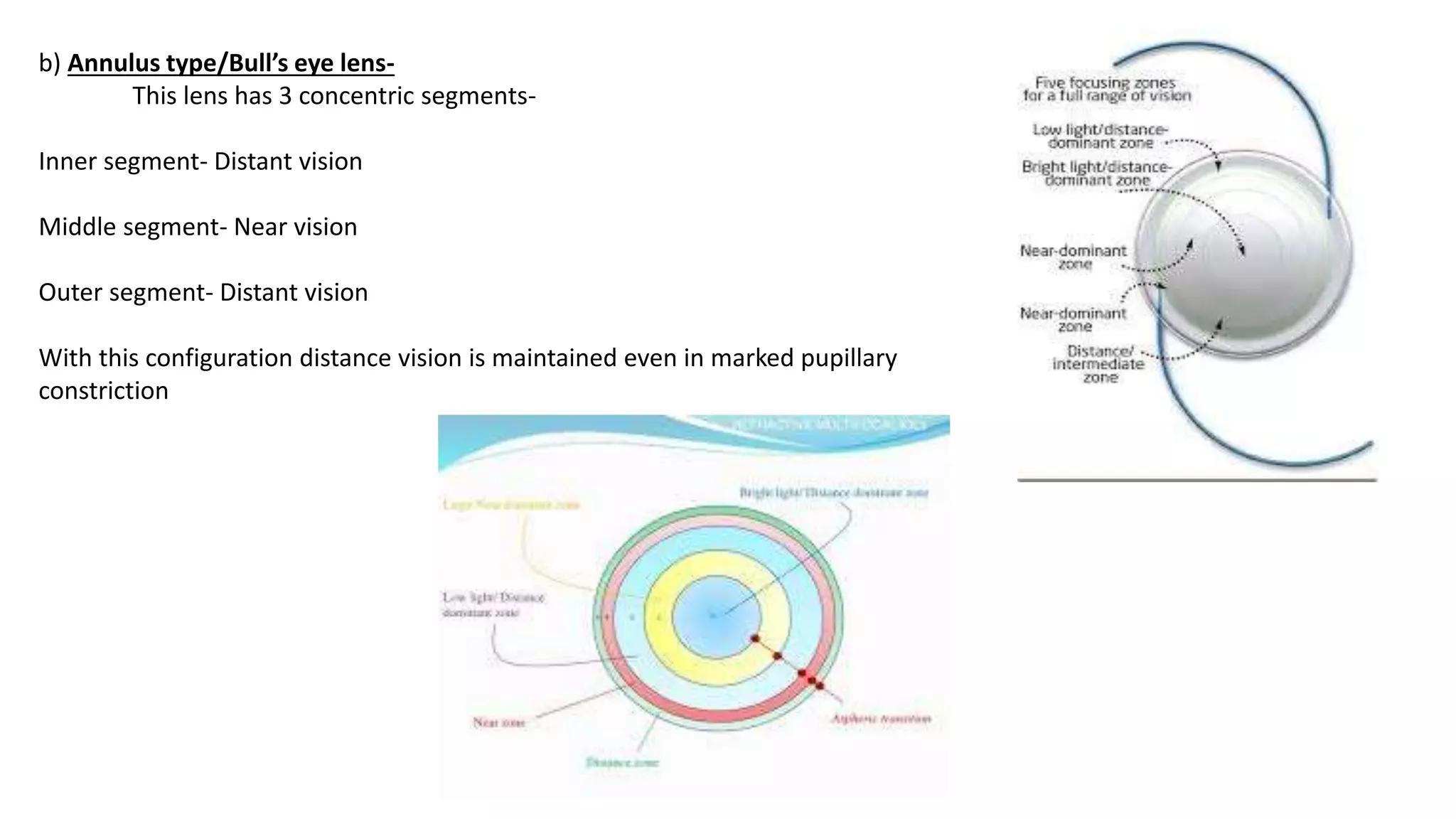
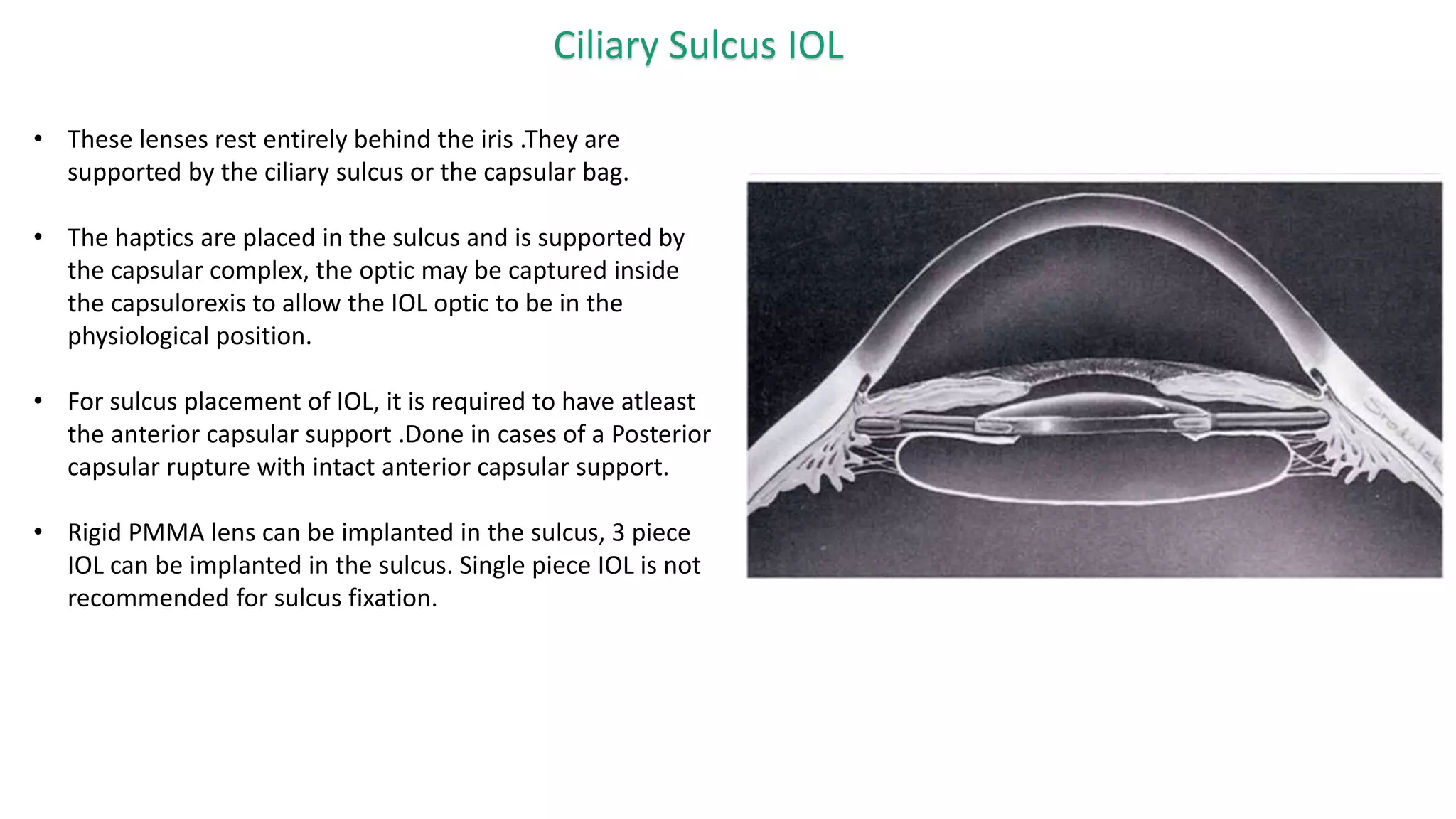
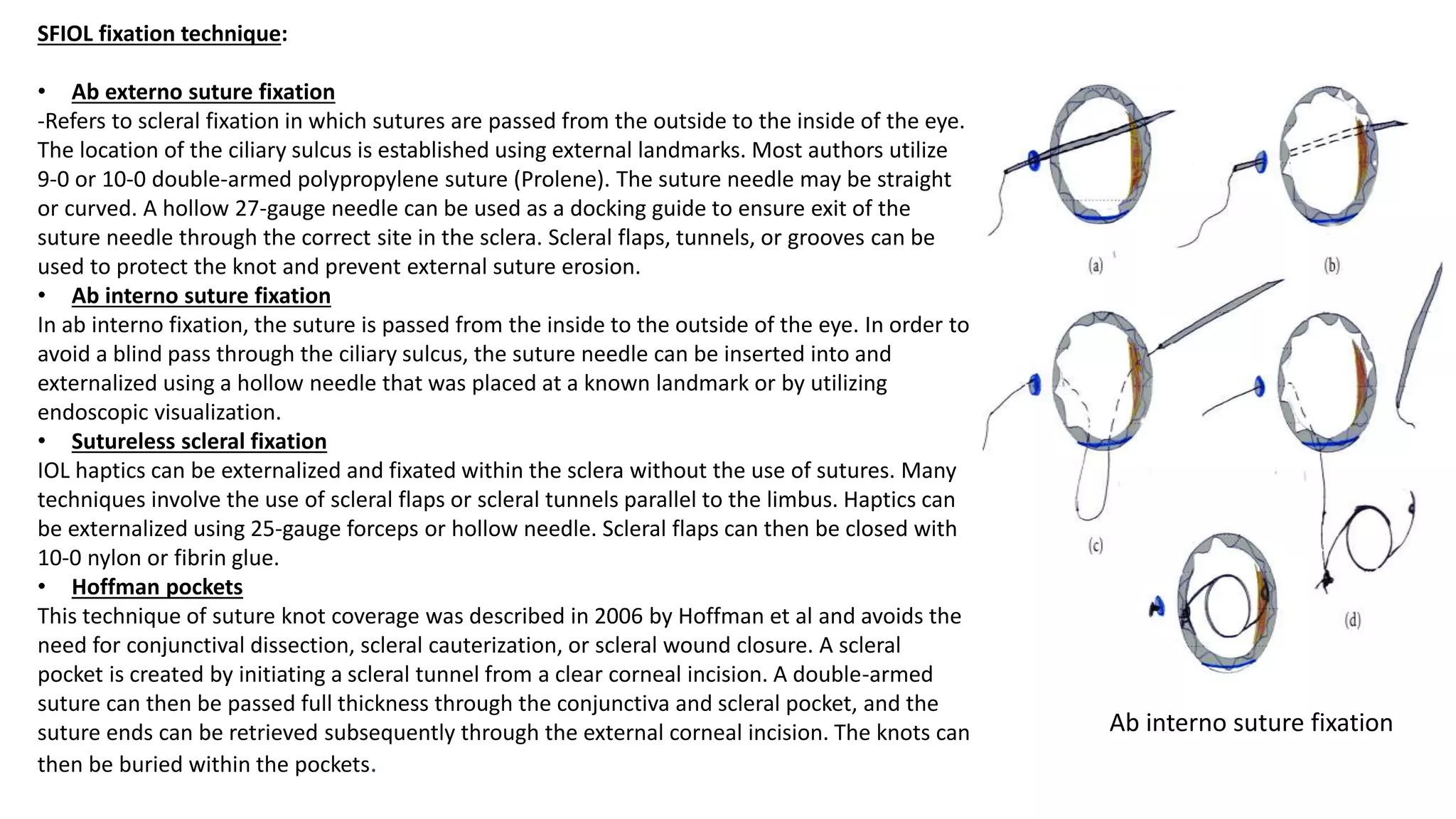
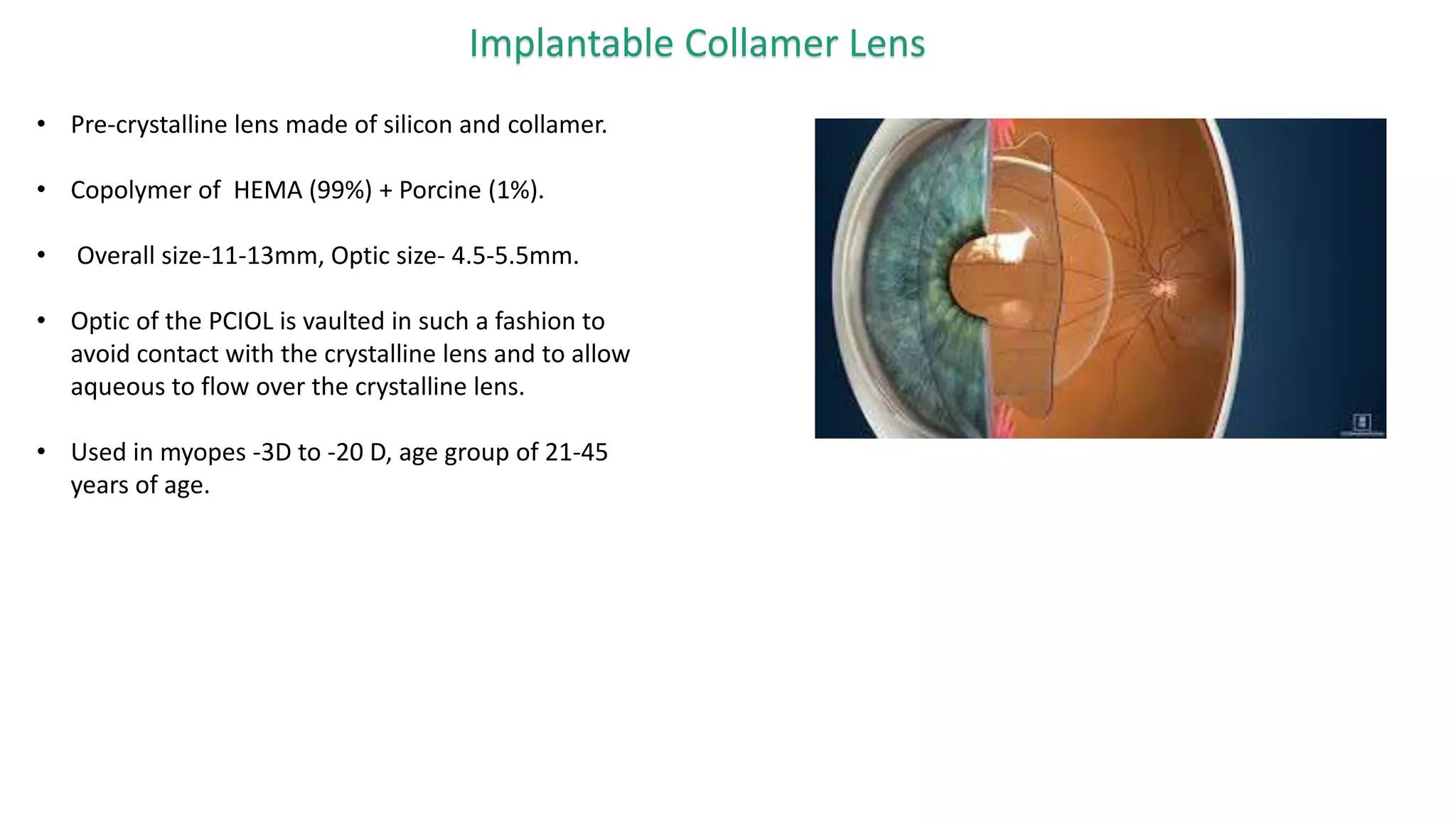
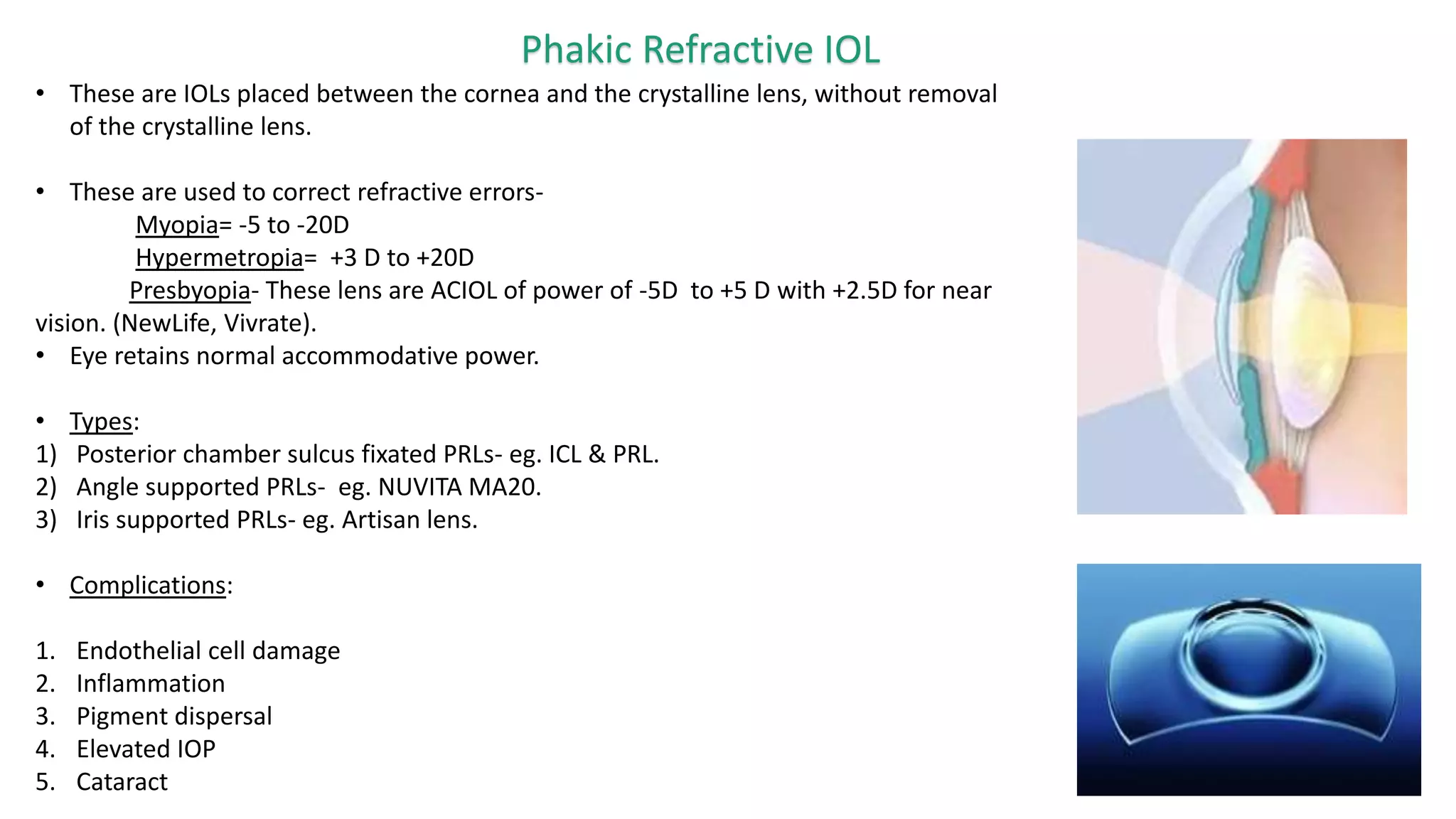
The document provides an overview of intraocular lenses (IOLs). It discusses the history and definition of IOLs, the generations of IOLs, parts of an IOL, IOL designs, materials, and properties. It also covers IOL placement sites, power calculation, complications like posterior capsular opacification, and recent advances in premium IOLs including multifocal, accommodative, and toric lenses.