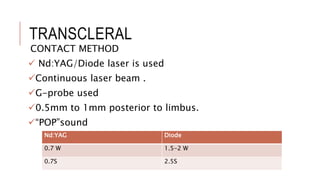
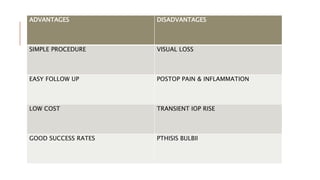
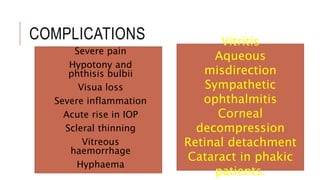
Cyclodestructive procedures reduce intraocular pressure by destroying ciliary processes in cases of refractory ocular pain and other severe glaucoma conditions. Various methods include cyclocryotherapy, laser cycloablations, and other techniques, each with specific indications and contraindications. While effective, these procedures may require multiple treatments and have a potential for significant complications, including vision loss and inflammation.