Downloaded 239 times

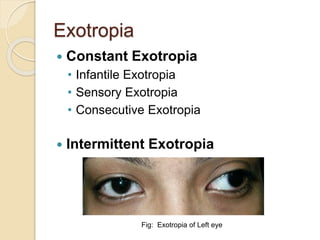






















Intermittent exotropia is the most common form of divergent strabismus where one or both eyes drift outward intermittently from normal alignment. It typically onset before age 5 and manifests during periods of inattention, fatigue, or drowsiness. Treatment options include non-surgical methods like spectacle correction, patching the dominant eye, or base-in prisms, as well as surgical recession of the lateral rectus muscles to improve alignment if control is lost. The goal of treatment is to restore proper eye alignment and preserve binocular single vision.























































































