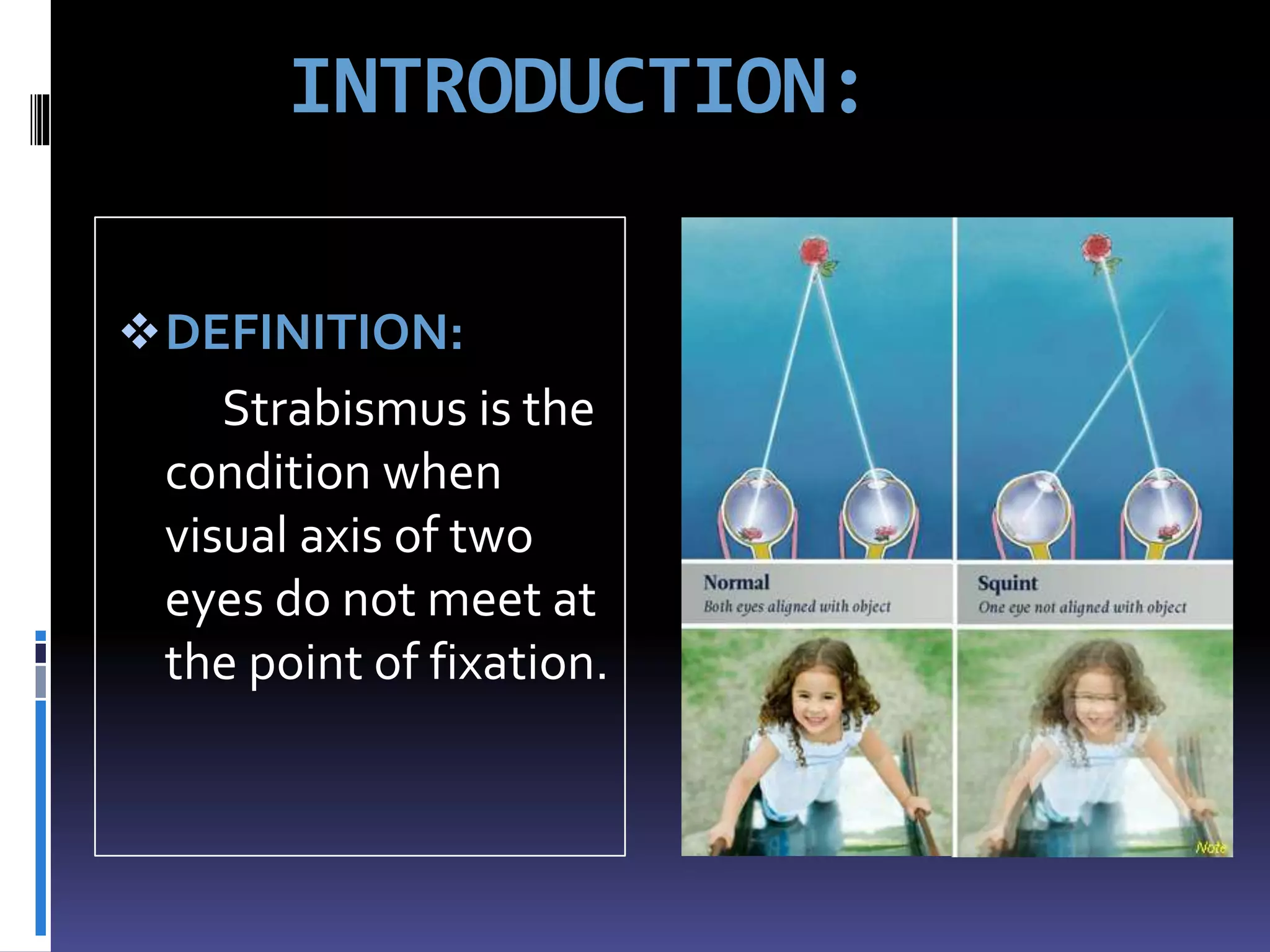
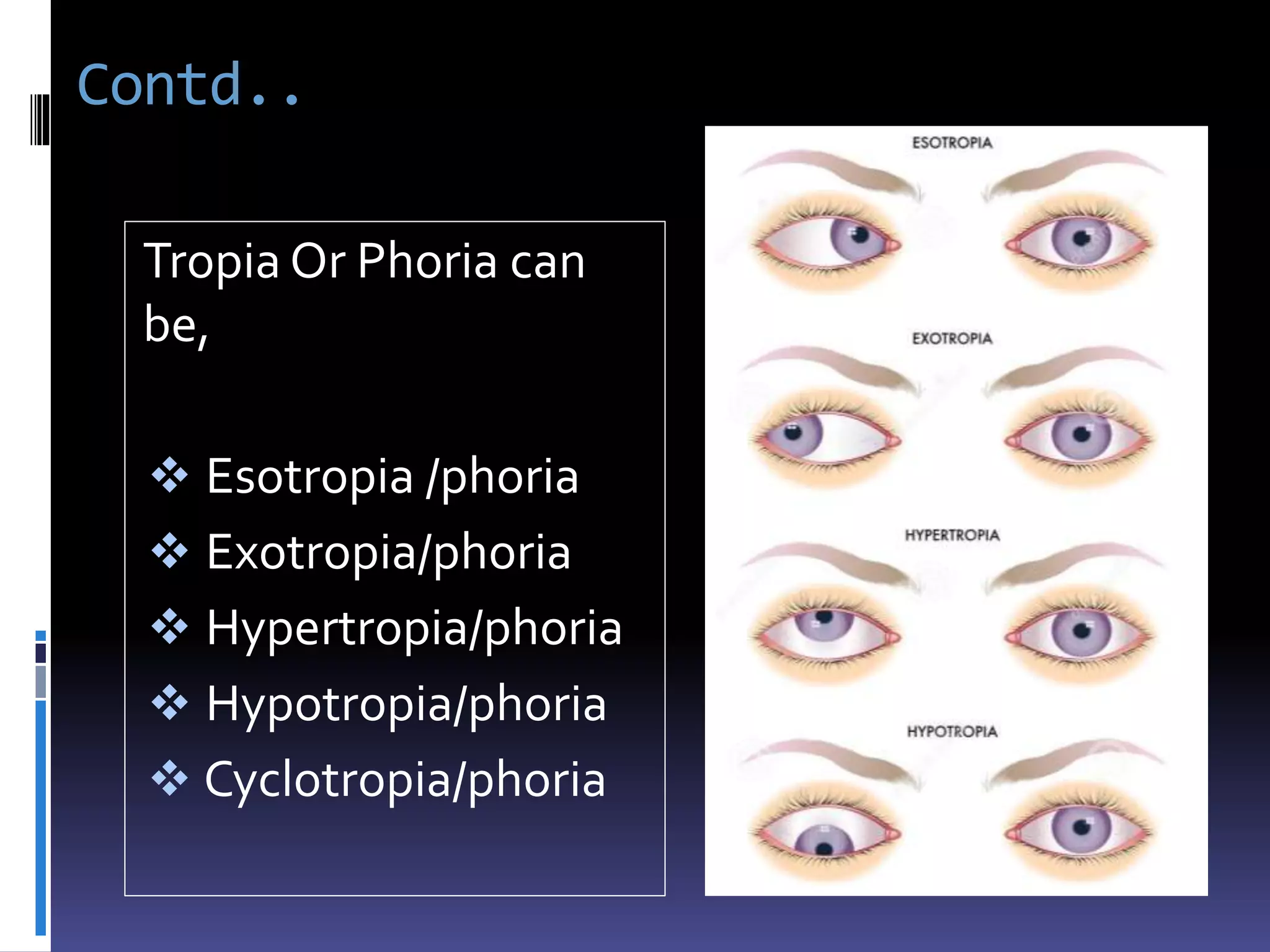
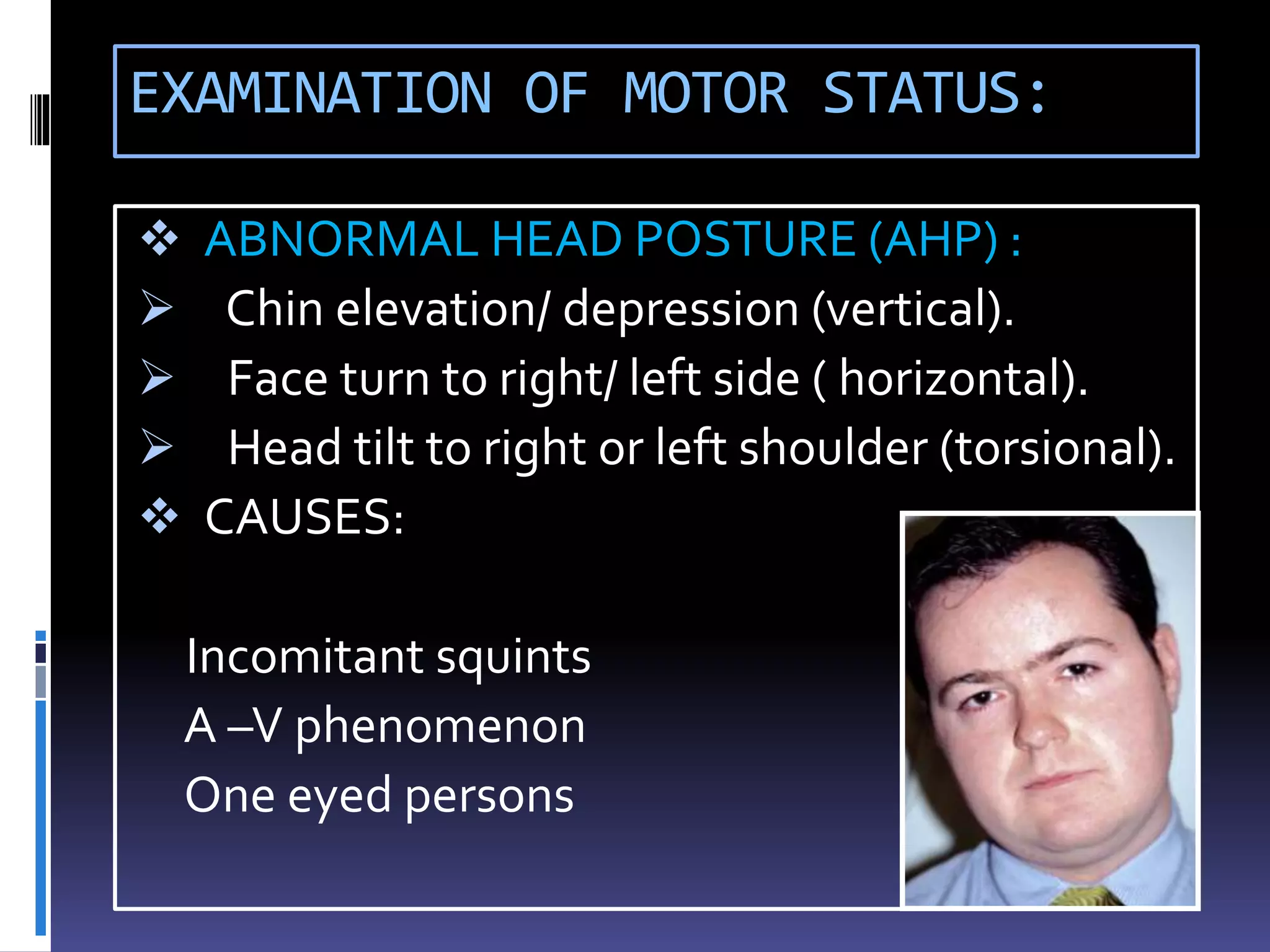
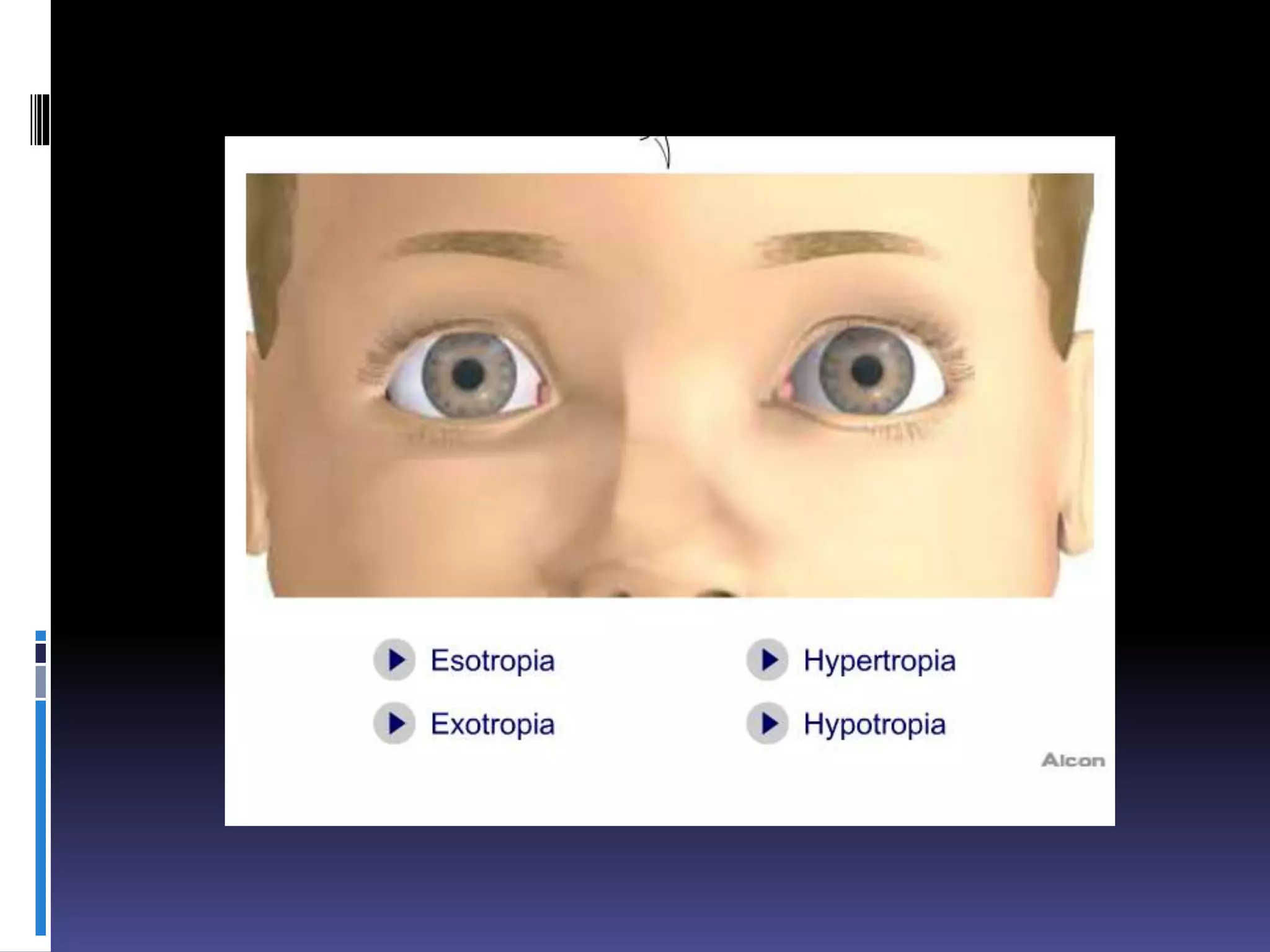
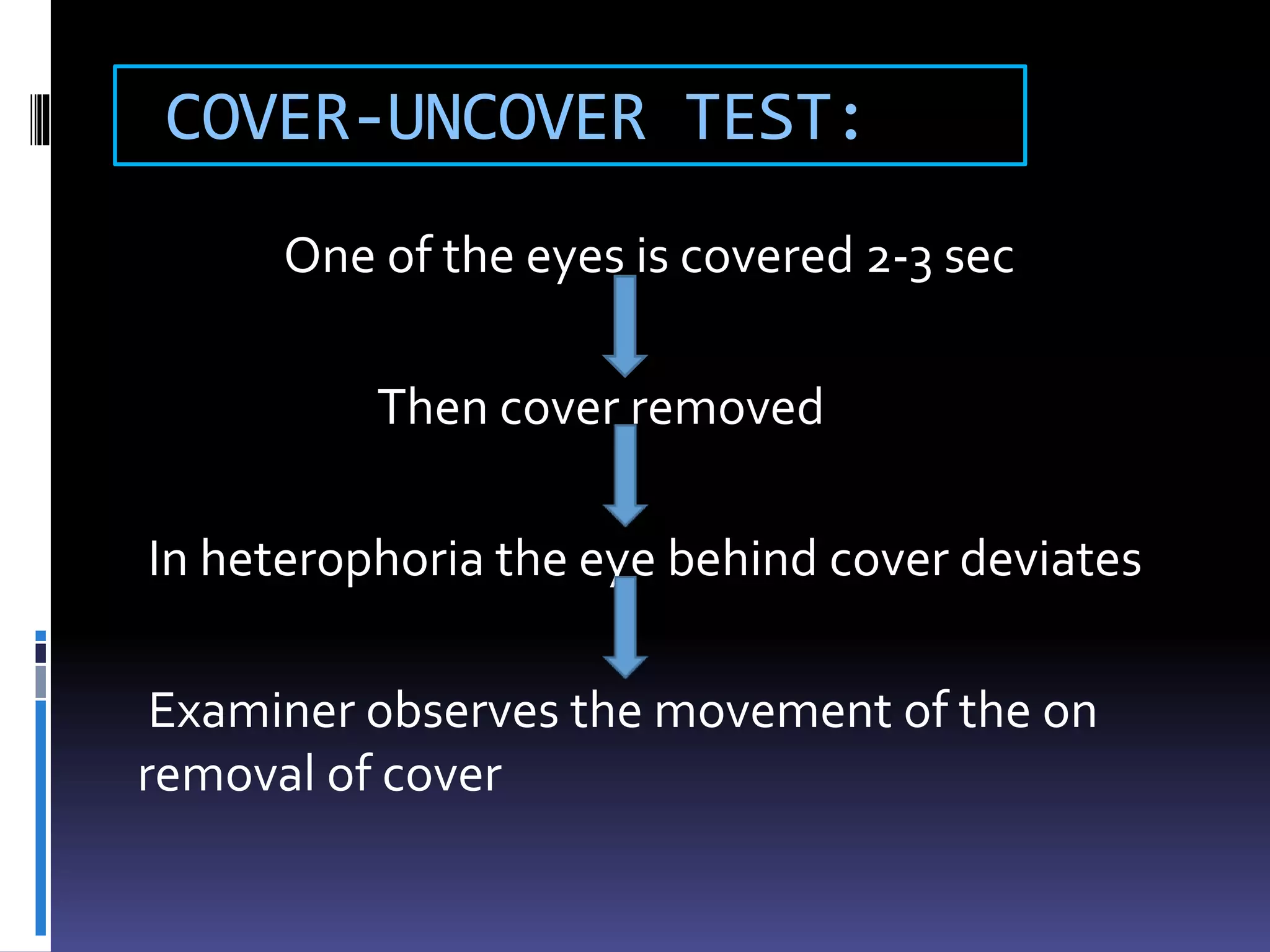
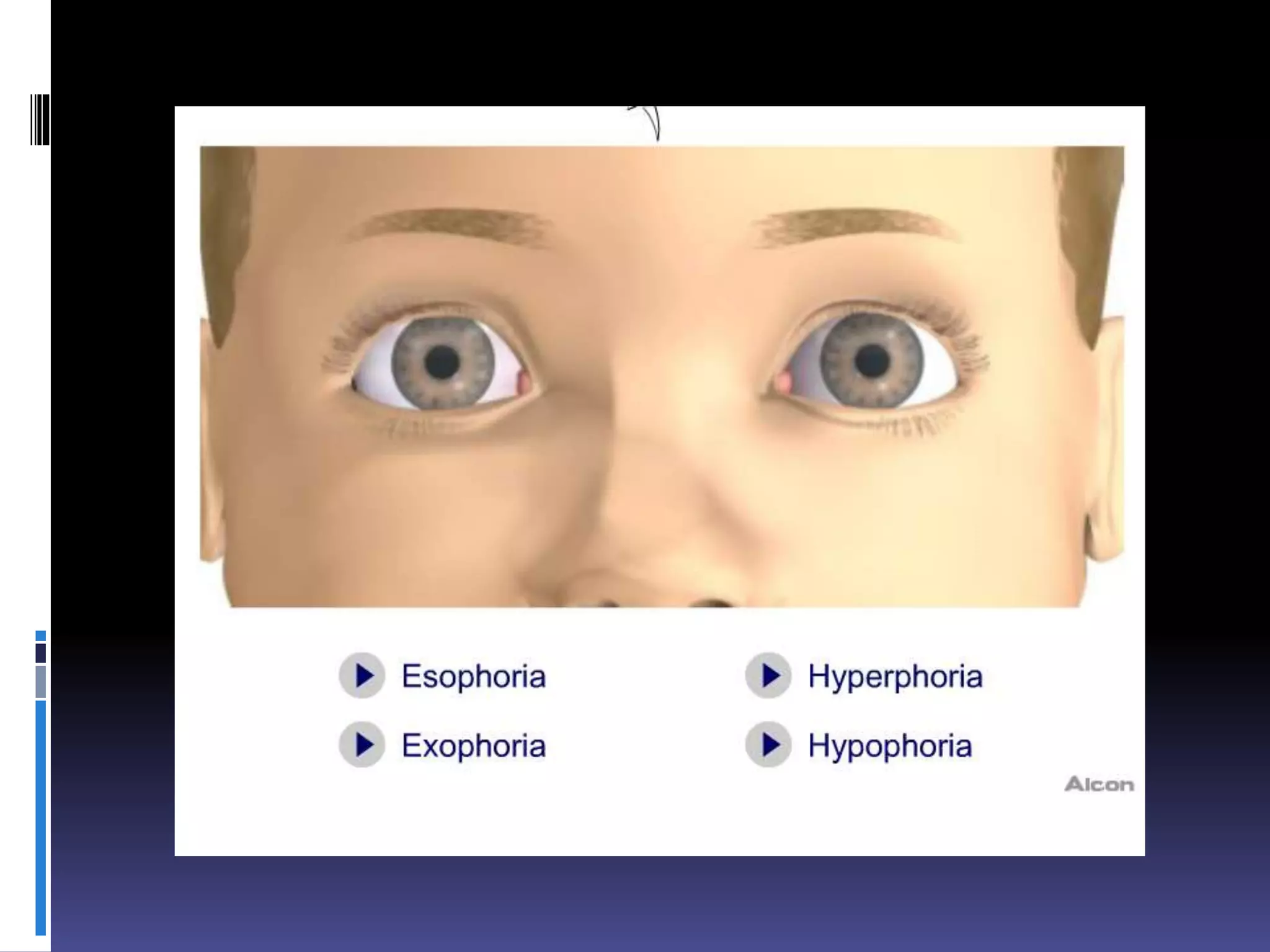
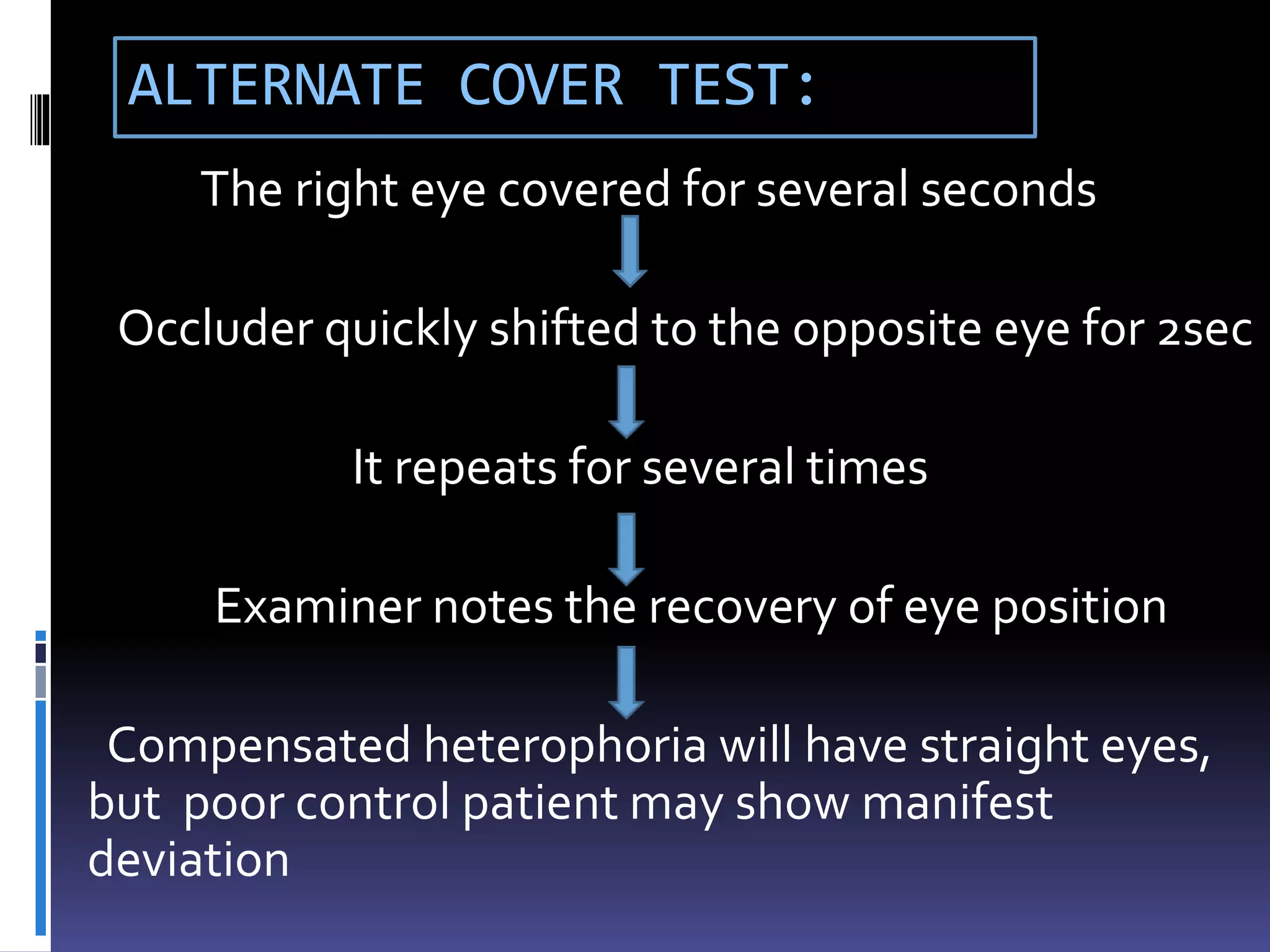
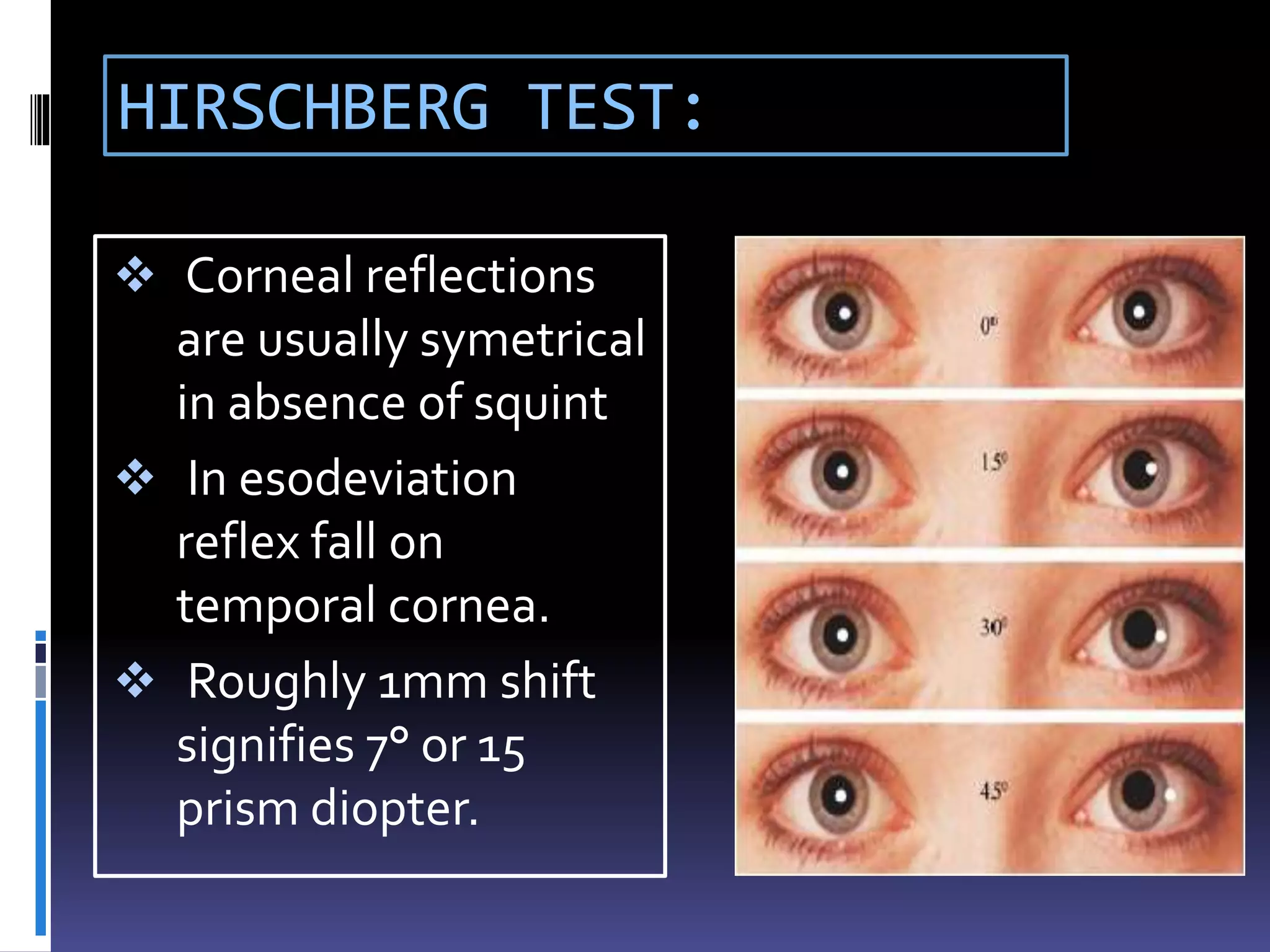
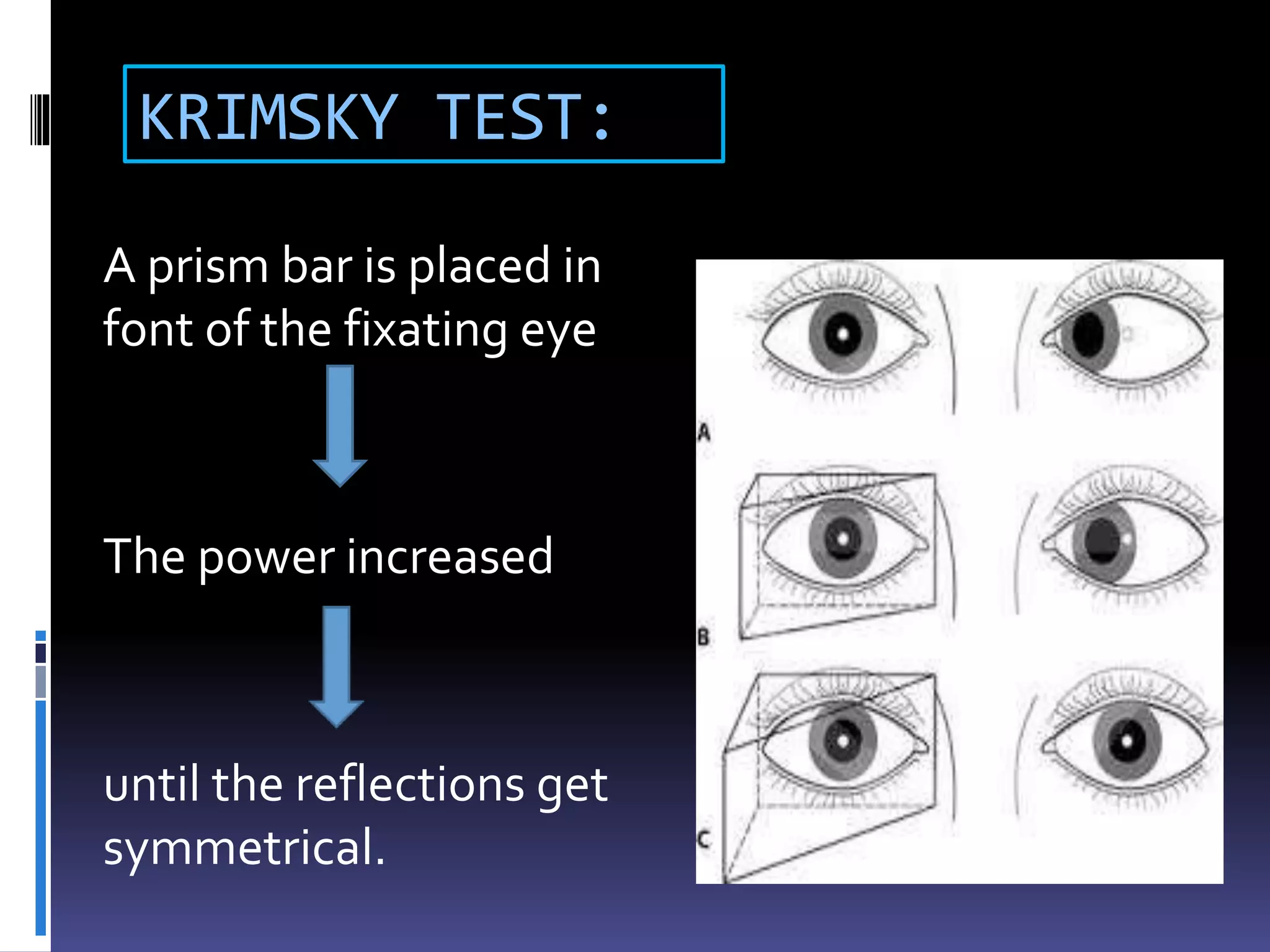
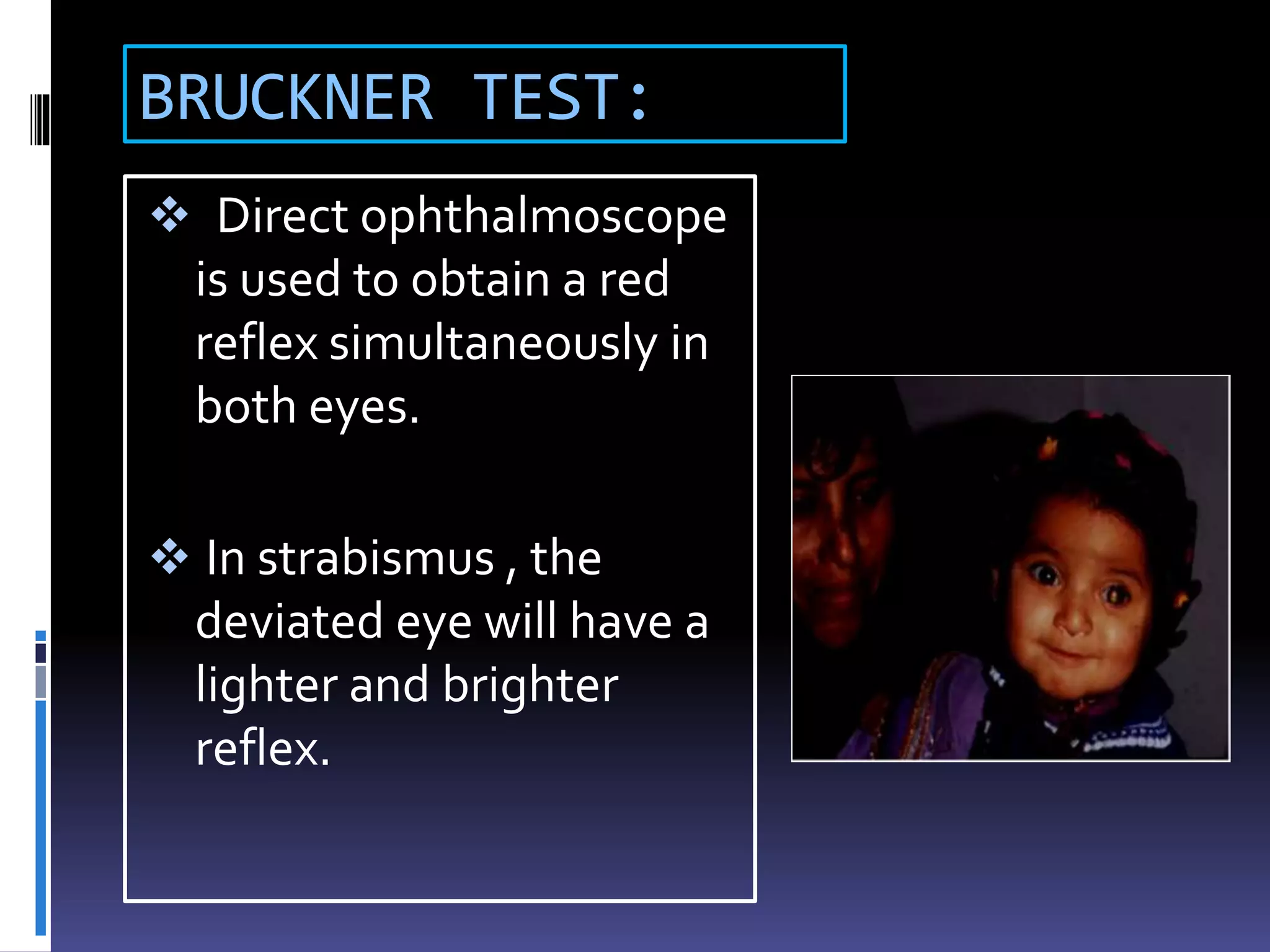
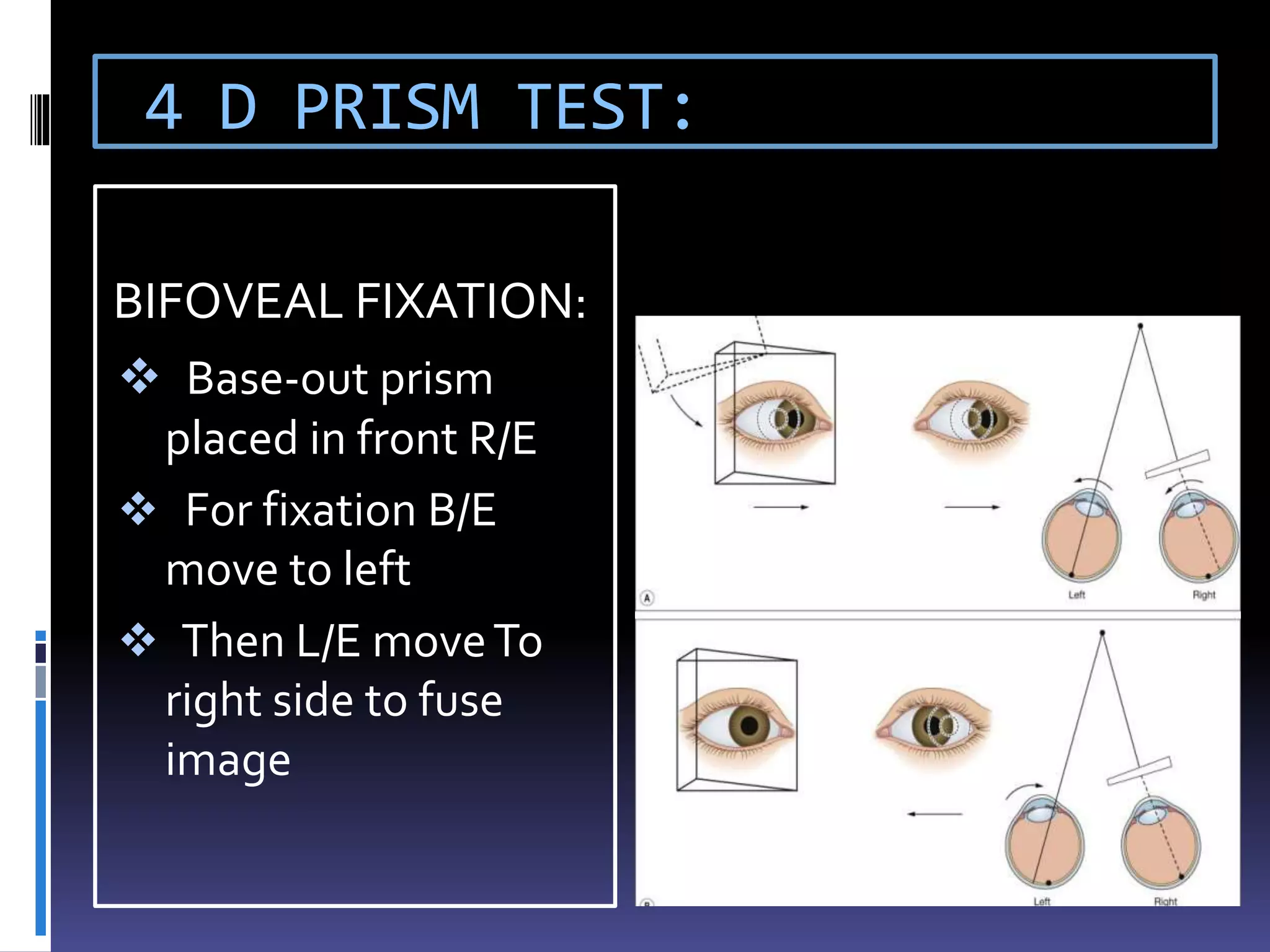
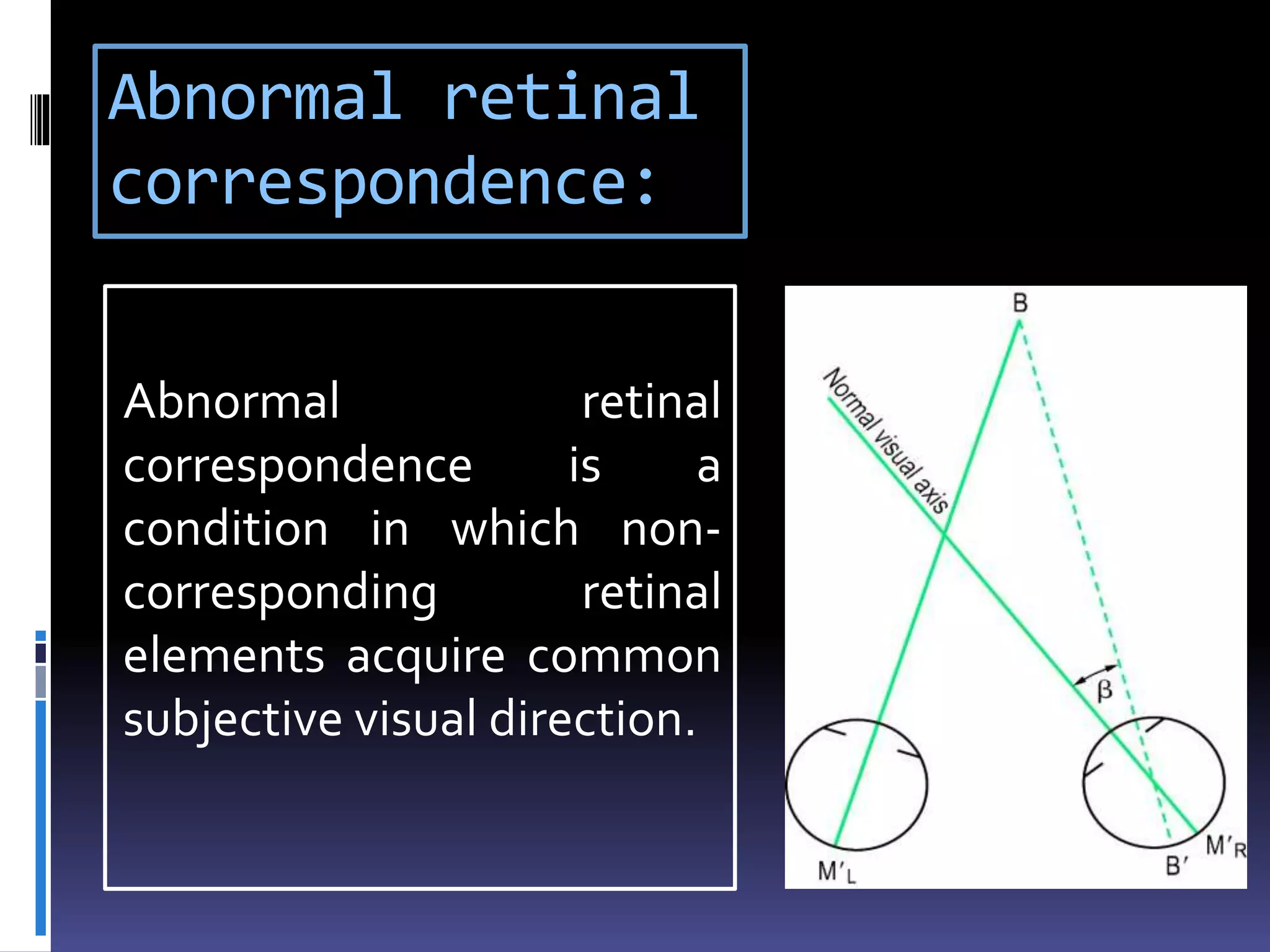
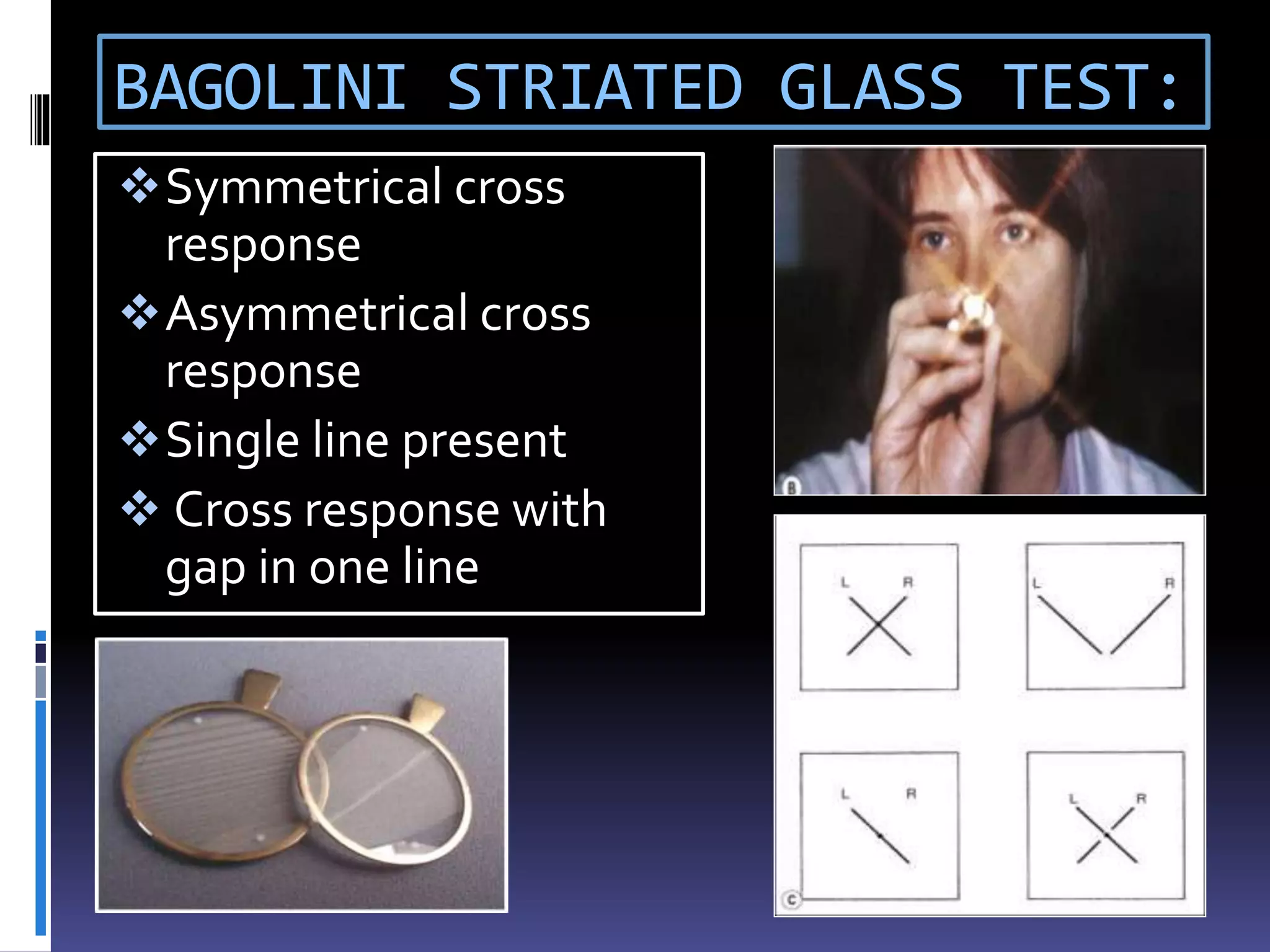
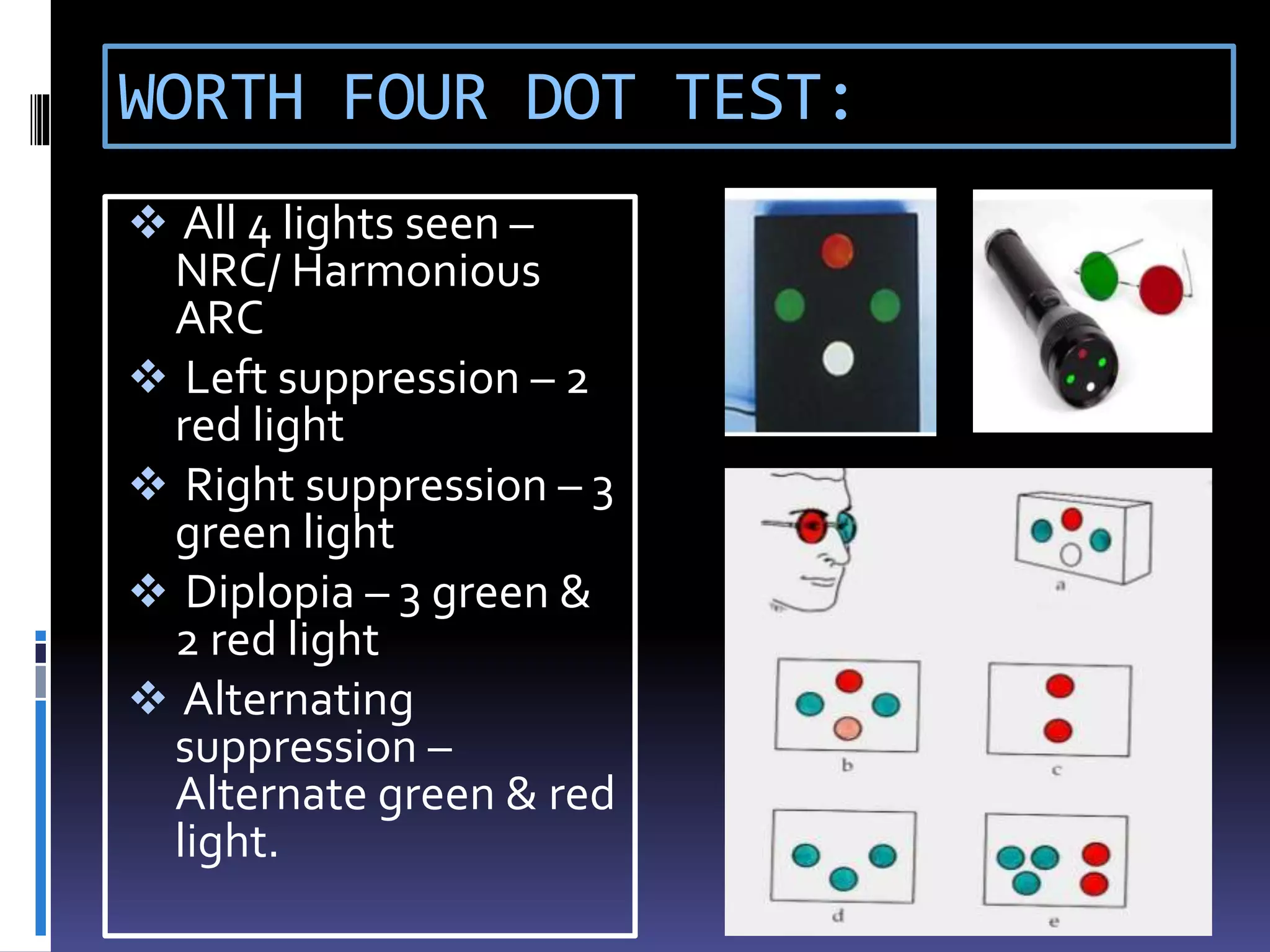
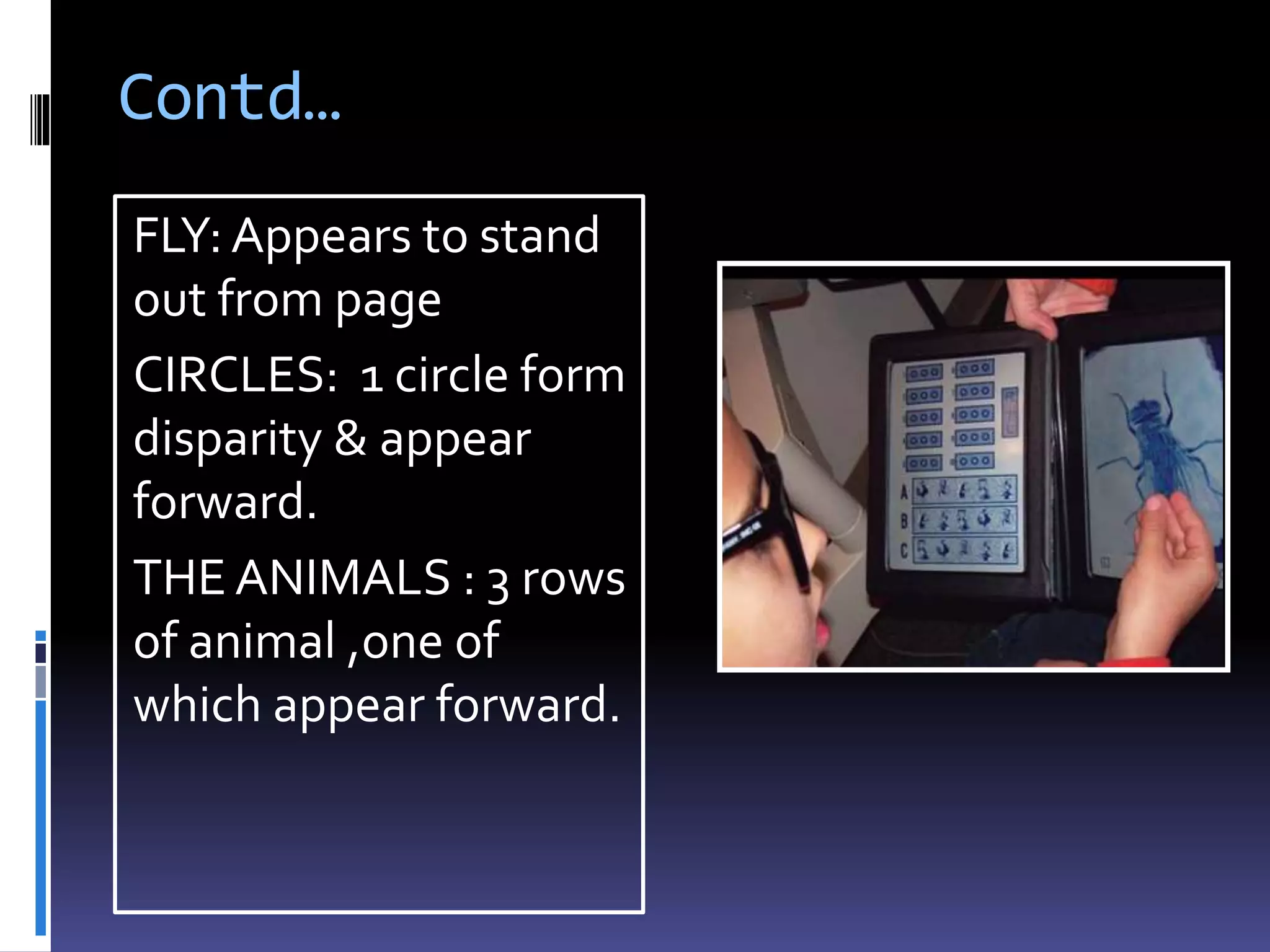
The document defines and describes various types of strabismus including tropia, phoria, comitant and incomitant deviations. It outlines the assessment of strabismus including taking a patient history, testing visual acuity, and performing an examination of motor and sensory status. The examination involves evaluating ocular alignment using tests such as cover testing, evaluating eye movements and fusion, and identifying suppression or abnormal retinal correspondence.