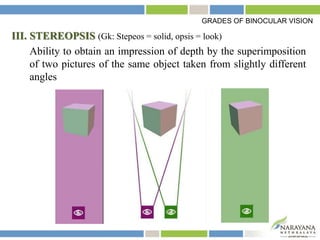
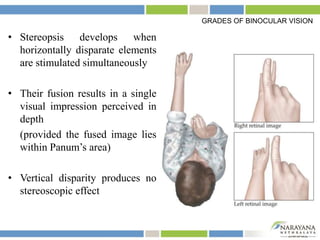
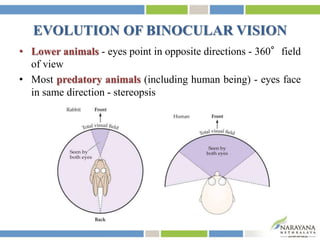

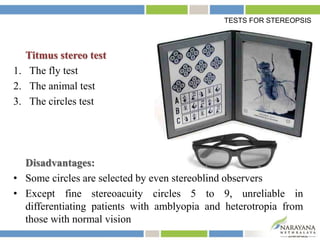
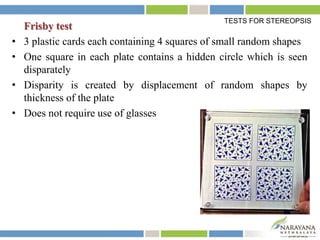
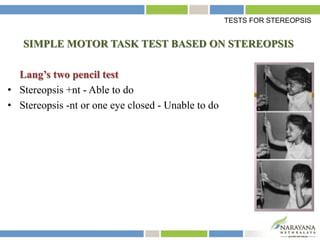


Binocular vision requires two clear eyes that can coordinate focusing on the same object. This allows the brain to fuse the two slightly different retinal images into a single image. There are grades of binocular vision including fusion and stereopsis, which is the ability to perceive depth. For binocular vision to develop, the eyes must maintain proper retinal correspondence and suppression. Tests like the Titmus fly test evaluate stereopsis. Understanding binocular vision and stereopsis is important for diagnosing and treating eye alignment disorders.

















































































